
View this report
Summary
- The Chief Medical Officer for England recommends that an alcohol-free childhood up to 18 is the safest option. The law states alcohol may only be purchased by people aged 18 or over, but the law on underage alcohol consumption is more complex.
- Drinking alcohol during adolescence poses a range of health and social risks, which means reducing it needs to be a policy priority.
- Despite recent declines, underage drinking remains prevalent across the UK. Particularly alarmingly a significant minority of adolescents consume alcohol at high levels – greater even than the adult low-risk guidelines.
- A complex array of interconnected factors are causally associated with underage drinking, and understanding these presents key potential policy targets.
- Underage drinking has declined in the UK, but there is some emerging evidence that this decline may be slowing and in parts of the UK may even have reversed.
Introduction
How much, what, where, when, and why people drink alcohol differs considerably across the lifespan. This is likely influenced both by changing social position and roles, and also by cohort – how you drink when you are young will influence how you drink when you are older.
The physical and social consequences of drinking also differ considerably, morbidity and mortality is more common in older groups, whether that’s from alcohol or other factors. Some groups face specific risks – underage people may be more vulnerable to setting long-term behaviours, working-age people will be at higher risk of work-based accidents, and older-people may be more vulnerable to chronic health consequences.
This series of briefings on alcohol through the life course will look at three different age groups: underage drinkers, young drinkers, and older drinkers. Understanding the patterns of drinking in different demographics matters as it enables us to identify risks and thus target policy solutions to particular groups.
What are the health impacts of underage drinking?
The Chief Medical Officer for England recommends that an alcohol-free childhood up to 18 is the safest option [1]. However, the law does not mirror that recommendation. In the UK it is illegal to [2]:
- Sell alcohol to someone under the age of 18;
- By or try to buy alcohol if you are under the age of 18;
- For an adult to buy or try to buy alcohol for someone under the age of 18.
If you are accompanied by an adult and aged 16-17 years of age you are allowed to drink (but not buy) beer, wine, or cider with a meal at a licensed premises. The law also permits children aged older than five to drink alcohol at home.
To align with how data is gathered in the UK most of the figures contained below relate to children aged 11-15. More on those aged 16-24 can be found in our briefing on alcohol and young people.
What is the law on underage drinking?
Harms faced by children and young people
Alcohol is a causal factor for over 200 diseases or injury conditions [3]. Children are vulnerable to harm not only from their own drinking but also due to alcohol consumed by others, be that through traffic accidents, neglect, or unintentional injury. This briefing focuses exclusively on the harms children face from their own consumption.
In 2009, the Chief Medical Officer for England published a review of the health and social consequences of underage drinking [4]. These risks are wide-ranging and include:
- Immediate risks such as injury, violence, suicide, risky sexual activity, and other substance use;
- Developmental risks for the brain, liver, skeleton, and endocrine system. In particular adolescence is a critical period in brain development and the effects of alcohol can lead to permanent consequences;
- Social risks, including an association with future involvement in crime and lower educational outcomes; and
- Worse future drinking patterns: earlier drinking and binge drinking is associated with heavier future drinking, binging, and alcohol dependence and abuse.
Measuring harms from underage drinking
Hospital admissions
Alcohol-specific admissions [5] for those aged under 18 have declined in England over the last ten years. This is in contrast to all alcohol-specific admissions, which have increased by around 35% over the same period [6]. The absolute number is still substantial however, with over 11,000 alcohol-specific admissions among under 18s in the most recent three-year period [7].
Figure 1 Admission episodes for alcohol-specific conditions
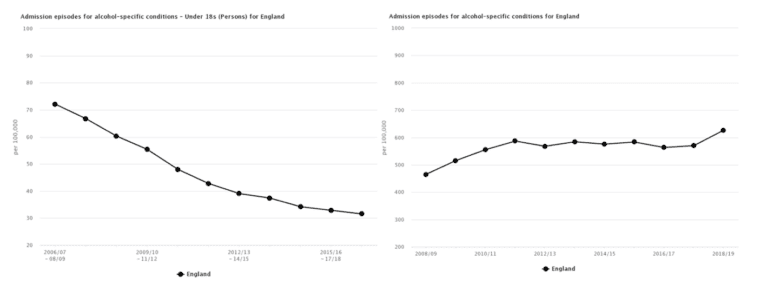
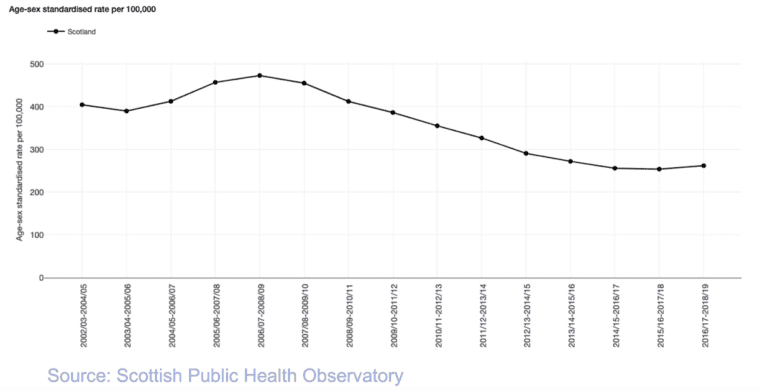
In Scotland, the closest equivalent statistic is alcohol-related (a different criteria to alcohol-specific) hospital admissions for those aged 11-25 [8]. This has declined over a similar period, but may be beginning to increase again.
Figure 2 Alcohol-related hospital admissions, aged 11-25 years
Time-series data is not readily available for Wales and Northern Ireland.
Social consequences
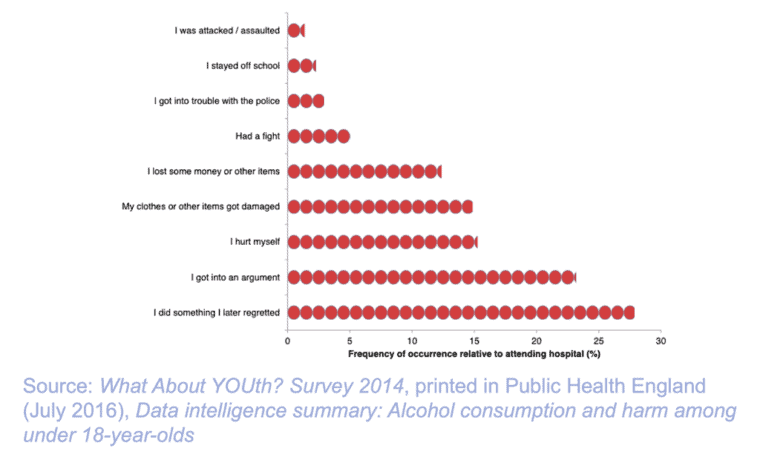
Hospital admissions represent the sharp end of the harm young people face. Public Health England demonstrated this using data from a 2014 survey [9]. It described how frequent a specific negative outcome is among children relative to hospital admission (eg getting into trouble with the police due to alcohol consumption is nearly three times as likely as being admitted to hospital).
Figure 3 Consequences of alcohol intake relative to hospital attendances, 15-year-olds who were drunk in the last four weeks
Pattern of underage alcohol use in the UK
Given the range of negative consequences outlined above knowing the levels and patterns of underage drinking in the UK is critical. There are different ways of measuring underage drinking that this briefing will look at: whether children have ever drunk alcohol (‘ever drinkers’), how often they drink, and the amount they drink.
Sources
The different constituent components of the UK gather data differently. This work will mainly make use of the 2018 NHS Digital Smoking, drinking, and drug use among young people in England (SDD, ages 11-15) [10], the 2018 Scottish Schools Adolescent Lifestyle and Substance Use Survey (SALSUS, ages 13 and 15) [11], the Welsh 2017/18 Health Behaviour in School-aged Children Survey and School Health Research Network Student Health and Wellbeing Survey (ages 11, 13, and 15) [12], and the 2016 Northern Irish Young Persons’ Behaviour and Attitudes Survey (YBAS, ages 11-16) [13]. Brief details of these surveys can be found in Annex A.
Children who have ever drunk alcohol
Prevalence
Across the UK, ever drinking among children is fairly common and rises with age.
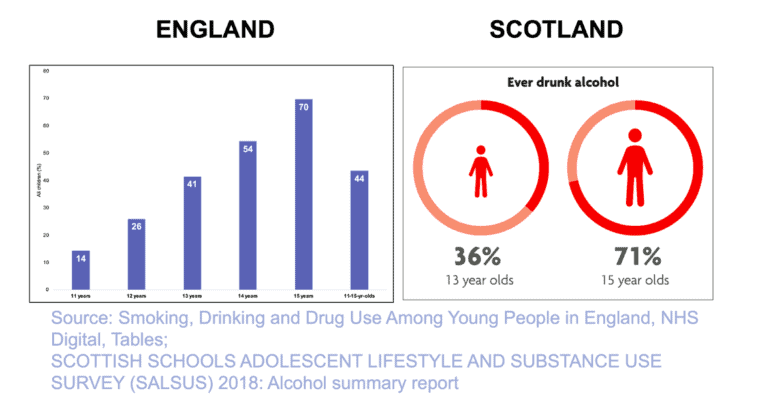
In England, 44% of children aged 11-15 have reported that they had ever had an alcoholic drink.
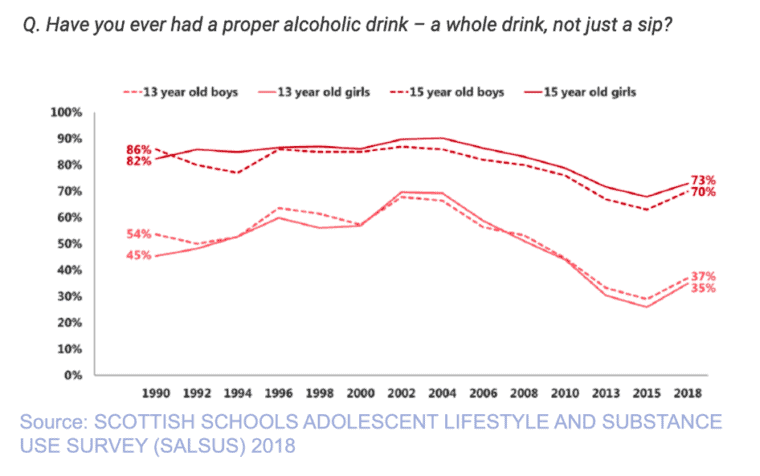
In Scotland, the equivalent number for 13-year-olds is 36%, rising to 71% amongst 15-year-olds.
In Wales, 51% of 13-year-olds have ever had an alcoholic drink, as have 77% of 15-year-olds [14].
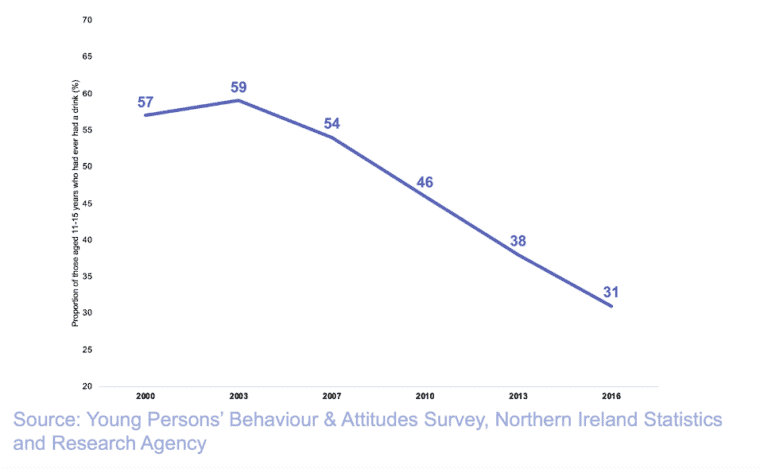
In Northern Ireland, one third of those aged 11-16 have ever drunk alcohol, half of whom had their first drink at under the age of 13.
Figure 4 Proportion of children aged 11-15 years who had ever drunk alcohol
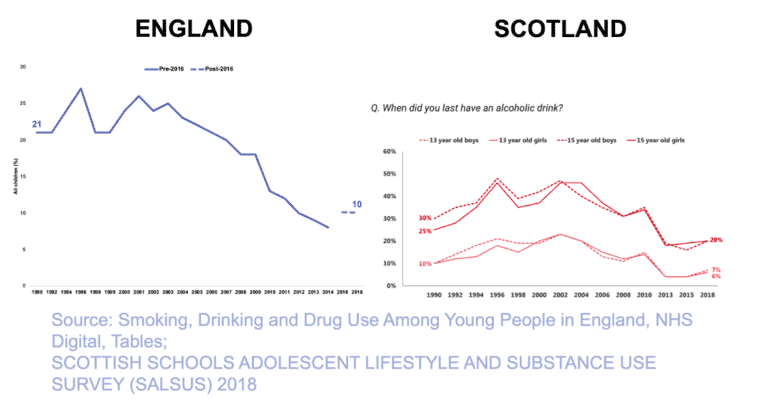
Changes over time
Until at least the mid-2010s the prevalence of children who have ever had a drink declined substantially across the UK. However, between 2016 and 2018 the prevalence increased in Scotland.
Figure 5 Proportion of pupils who have ever had a drink, by sex and age (1990-2018)
The most recent data for Northern Ireland – which also shows a decline over time – is prior to the 2016-18 increase.
Figure 6 Proportion of pupils who have ever had a drink, by sex and age (2000-2016)
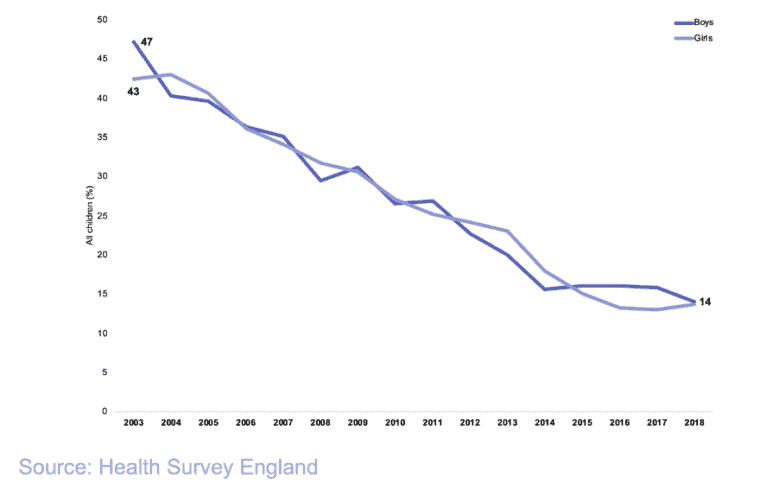
In 2016, England changed the survey question, interrupting the time series. Another data source, the Health Survey for England – which is for a different but overlapping age group (ages 8-15) – the rate of decline in ever drinking has slowed from 2015 onwards [15].
Figure 7 Ever drinking amongst 8-15-year-olds (2003-2018)
Time series data was not readily available for Wales.
How often do underage people drink?
Prevalence of regular and frequent drinking
Another way to measure underage drinking is to assess how often children drink, this can either be assessed by asking them how often they drink or asking them if they have had a drink in the past week (this latter group is referred to as ‘current drinkers’). As with ever drinking, regular and current underage drinking rises with age.
In England, 17% of 11-15-year-olds report drinking at least once a month. Amongst 15-year-olds alone this rises to 38%. Regarding current drinkers in England, 10% of those aged 11-15 had drunk in the last week, with 23% of 15-year-olds having done so.
In Scotland, 6% of 13-year-olds had drunk in the last week, whereas 20% of 15-year-olds had.
In Wales, around 8% of those aged 13 to 16 years drank at least weekly, rising to 17% of those aged 15.
In Northern Ireland, 26% of those aged 11-16 years who do drink alcohol did so a few times a month or more.
Trends in regular drinking
Similar to ever drinking, current drinking also declined in Scotland until at least the mid-2010s, with an increase in the latter half of the decade. The trend in England in the SDD was interrupted by the change in question, and this data is not available in the Health Survey for England. Trend data was not readily available for Wales or for Northern Ireland.
Figure 8 Trends in drinking in the last week, by age and sex (1990-2018)
What about 16-17-year-olds?
The Chief Medical Officer for England recommends that an alcohol-free childhood is the healthiest option [16]. However, we know that the likelihood of consumption rises with age: in England in 2011-14 by age 17 64% of boys and 48% of girls had drunk alcohol in the past week (analysis of the Health Survey for England by Public Health England) [17]. You can read more about the 16-24 year age bracket in our briefing on alcohol and young people.
National and international comparisons
As discussed earlier, making comparisons between different countries is challenging as survey methodologies differ. The WHO Europe figures, which were discussed above for Wales and are from 2017/18, do include multiple countries, including Scotland and England. The prevalence of current drinking (had a drink in the last 30 days) and lifetime drinking in Scotland, Wales, and England are all above the average of the countries surveyed (45 countries, mostly, but not exclusively, in Europe) [18].
How much do underage people drink?
Amount of alcohol consumed
How much children are drinking can be measured by estimating units consumed, however outside England data on units consumed per week is less readily available. Information is collected on the experience of being drunk, which will also be presented in this section.
In England, those who had drunk alcohol in the last week had consumed an average of approximately 10 units that week. Concerningly, one in five (21%) had consumed more than the CMOs’ low-risk adult guidelines (14 units or more). In Wales, just over half of those who drink alcohol consume more than one drink on the days that they drink, and 19% drink five or more.
Experience of being drunk
In England, 9% of those aged 11-15 had been drunk in the last four weeks.
In Scotland, 53% of 13-year-olds had ever been drunk, as had 70% of 15-year-olds, and around half of those who had drunk in the past week, in both age groups, had also been drunk in the past week.
In Wales, 22% of those aged 11-15 had been drunk, 10% in the last 30 days. 9% had been drunk at least four times in their life.
In Northern Ireland, 45% of those who reporting having ever drunk alcohol report having been drunk, and over 30% have been drunk two or more times.
Underage drinking: what, where, when, and why?
The most comprehensive data on what, and how, young people drink is relates to England and is from the 2018 NHS Digital SDD [19], which is where all of the figures below are from unless otherwise stated.
What do underage people drink?
Amongst those who drunk in the last week beer, lager, or cider was most commonly consumed amongst boys. Girls were more likely than boys to have drunk spirits, wine, martini, sherry, or alcopops.
Where do they get alcohol from?
It is most common for underage people to get alcohol from home, relatives, or friends. A small, but non-negligible fraction buys alcohol from shops. This fraction rises amongst older children. These patterns are also seen in Scotland.
Where do they drink?
Underage drinking most commonly occurs at home, followed by parties with friends or at someone else’s home. Drinking in pubs or bars was uncommon. A similar pattern is seen in Scotland, however drinking on the street occurs relatively more frequently (although still outside the top three).
Who do they drink with?
Parents are the most common people underage people drink with, followed by friends, then other relatives. In the older age groups, drinking with friends is more common.
Do young people think it is okay to drink?
Until recently, the acceptability of drinking amongst young people had been falling, but it appears to be rising again. Four in five (79%) of Scottish 15-year-olds think it’s okay to try alcohol, and just under half (49%) think it is okay to get drunk. In England, nearly half (47%) of 15-year-olds think it is okay to drink alcohol once a week and almost one in five (19%) think it is okay to get drunk once a week.
Why do young people think their peers drink?
The top three reasons young people give as to why their friends drink are all peer-group related: to look cool, due to pressure from friends, and to be more sociable.
Factors that drive underage drinking
The following contains a short summary of some key factors associated with underage drinking. A wide array of studies and analysis have been carried out into the causes of underage drinking. Evaluating this plethora of information to make statements about causal factors, which could make potential policy targets, is challenging. This section highlights some of the key associations identified in national surveys in the UK, and from reviews that may be of policy relevance. It is not an exhaustive list of all associations with underage drinking. A more detailed discussion of the factors below, their selection, and the sources used is available in Annex B.
Sociodemographic factors
- Age: older children are more likely to drink across the UK.
- Religion: religion has been shown to have a lower likelihood of drinking, particularly among those who identify as Muslim.
- Ethnicity: Children of white ethnicity are more likely to drink than children belonging to other ethnic groups.
- Socioeconomic status: while there is some evidence that more advantaged children are more likely to drink, there are not clear patterns and these do not persist across the UK.
- Gender: unlike adult drinking, where men drink more than women, there appear to be minimal differences by gender in underage drinking.
Family factors
- Parental provision of alcohol: this is controversial, with many people believing that exposure in a controlled home environment may be safer. However, there is clear evidence that in cultures such as the UK where there is a tolerance towards binge drinking, the provision of alcohol at home has negative implications for a child’s pattern of underage drinking;
- Favourable parental attitudes towards drinking are causally linked to increased underage drinking;
- Parental alcohol use: there is some evidence that seeing parents drunk is associated with underage alcohol use;
- Parental monitoring, support, involvement, and a good parent-child relationship all seem to be protective factors for underage drinking;
- Single parent families: children from single parent families are more likely to drink, however, this association is likely to be explained by other factors such as reduced resources, rather than the structure of the family itself [20].
For more information about family influences see the Institute of Alcohol Studies 2017 report Like Sugar for Adults.
Peer factors
Children report that peer factors are major influences on their drinking. Peer influence is associated with alcohol consumption, but this relationship may be mediated in part by other factors. Families might influence who a children’s peers are, and children may themselves self-select for peers with similar drinking habits to themselves [22].
Individual health and social factors
- A number of negative experiences at school are associated with alcohol use.
- Poorer emotional and mental wellbeing, and behavioural problems also associate with alcohol use.
- Other health behaviours: smoking, drug use, and poorer self-reported health can associate with underage drinking.
Population level factors
In addition to the individual-level factors described above, population-level factors are also important influences as to whether young people drink (as with adults). The World Health Organization identifies three ‘best buys’ as policies that have the greatest impact on alcohol harm, for the lowest cost, each of which are discussed briefly below [23].
Marketing: Exposure to alcohol marketing makes children more likely to start drinking and, if they are already drinking, to drink more [24]. A recent large study found that four in five young people (aged 11-19) had noticed alcohol marketing in the past month, with half of those aged 11-17 being exposed to 28 or more instances of alcohol marketing in that period [25].
For further information, see our briefing on alcohol and marketing.
Price: This is a key policy, recommended by the WHO, as a way of reducing underage drinking [26]. For more information, see our briefings on the price of alcohol.
Availability: As it is illegal to purchase alcohol underage, access for children will often depend largely on the provision of alcohol by others (more on enforcement of age limits is discussed later). The work from the Joseph Rowntree foundation identified availability as one of the five key factors influencing underage drinking.
Reasons for the trend in underage drinking
The trend
There is has been a clear downward trend in underage drinking in the UK, with similar changes seen elsewhere around the world. As described above in the 2016-2018 period a rise in children having ever drunk alcohol and children regularly drinking alcohol was seen.
In England, a change in question makes this more difficult to evaluate but the decline appears to have plateaued amongst 8-15-year-olds. This context makes understanding the causes of the decline critical to inform policy, especially as additional action may be needed to preserve this positive trend.
The Institute of Alcohol Studies published a report, Youthful Abandon in 2016 which examined the evidence for a number of possible causes. More recently, in 2018, the University of Sheffield launched a four-year project to evaluate the causes for the trends in underage drinking in England [27].
At the current time there is insufficient evidence to clearly identify the factors that drive this trend. Those discussed in Youthful Abandon are outlined briefly below, and where relevant new data is considered, further discussion and analysis can be found in that original report.
In short, while there are a range of plausible factors that might have driven this substantial trend there is not yet enough evidence to conclusively evaluate their role [28].
Youthful Abandon investigated the following explanations for this trend:
- Technology. In recent years technology has transformed the experience of young people perhaps more than any other group. There are reasons to think this might be protect against drinking (more concern about image, reduced face-to-face socializing where drinking may have occurred) or promote it (eg greater exposure to online alcohol marketing). At this stage, the links between this transformation and alcohol use remain unclear [29].
- Changing social norms. There are numerous possible changes in social norms that could plausibly reduce alcohol consumption. The acceptability of drinking in England amongst young people does appear to have declined, although notably the most recent evidence indicates that attitudes towards it may be softening again.
ACCEPTABILITY OF DRINKING, ENGLAND
- Change in parenting. Family factors have important causal relationships with underage drinking. Those aged 25-44 are drinking less than they used to: in England in 1998, 71% in that age group had drunk alcohol in the last week but this dropped to 58% in 2018 [30]. Parents may be more aware of their children’s activities, and also have closer, more open, relationships. Parents also appear to have become less tolerant of their children drinking, however recently there is some evidence that this attitude may be softening.
PARENT DOESN’T LIKE CHILD DRINKING
- Demographic changes. There have been substantial demographic shifts in the UK, with a fall in the proportion of people who identify as White [31] – this is also the group most likely to engage in underage drinking. However, the rates of underage drinking have declined across all ethnic groups [32]. It is plausible that a peer effect may be at work, where children with friends who don’t drink are less likely to drink themselves, thus allowing demographic changes to impact drinking amongst all groups.
DRANK LAST WEEK BY ETHNICITY, ENGLAND
- Economic effects. Affordability is a key driver of alcohol consumption, and there is some evidence that the price of alcohol, relative to the money an 11-15-year-old might have (the age group studied in the SDD), rose. The figure below, updated from Youthful abandon, plots the change in the RPI of beer and wine and spirits and the change in the 16-17 minimum wage (as a proxy of the amount of money 11-15-year-olds might have access to) [33]. During the decline in underage drinking the RPI of alcohol does appear to have outpaced the 16-17 minimum wage. Interestingly, recently this gap has narrowed. Further, aside from a direct impact worse economic prospects may also affect underage drinking – if it is viewed as a barrier to accessing a more competitive job market it may be avoided.
MINIMUM WAGE OF 16-17 YR OLDS AND RPI OF ALCOHOL
- Happier, more conscientious children. Poorer emotional wellbeing appears to associate with underage drinking, thus happier children may drink less. However, while from 1994-2007, children’s subjective wellbeing improved [34], however from 2009/10-2016/17 – a period of time when alcohol use was still falling – there has been a significant decrease in children’s rating of their overall happiness [35].
- Better legal enforcement. Those aged 11-15 rarely purchase alcohol from off- or on-licenses directly. Thus, while there have been a number of policy measures taken in this area it is likely that, at best, this could explain a small fraction of the change.
Annex A: Information on the data used
The components of the UK use different sources of data, with the key ones used in this work outlined below. The methodology of these studies differs, which can have significant implications for their findings. As such, they largely cannot be used to compare across the UK.
England
Date: 2018
NHS digital’s Smoking, drinking and drug use among young people in England (SDD) is a survey of 11-15-year-olds is conducted biennially (age is based on year at school, so may not perfectly match for all participants). In the most recent survey 13,664 children from 193 different schools participated under ‘exam conditions’ and confidentiality was highlighted. Full details of the methodology can be found in the footnote [36]. An additional source of data is the Health Survey for England. This is carried out in individual’s homes, potentially reducing the reporting of sensitive topics such as underage alcohol consumption [37].
Scotland
Date: 2018
In Scotland, there is the Scottish Schools Adolescent Lifestyle and Substance Use Survey (SALSUS). This has been carried out in Scotland since 2002 (prior to that Scotland was covered in a pan-UK survey). It again takes place in classrooms under exam conditions, with 13-year-olds and 15-year-olds (like the England survey it’s based on class, so not everyone will be precisely the same age). 21,650 people participated from 199 schools. Full details available in the footnote [38].
Wales
Date: 2017/18
In Wales, data is available from the World Health Organization’s Health Behaviours in School-Aged Children (HBSC). This has been combined with a broader piece of work – the Health Behaviour in School-aged Children Survey and School Health Research Network Student Health and Wellbeing Survey [39]. In general, this briefing will use figures presented in the report from the second piece of work, if they are unavailable the HBSC report will be used. A total of 103,971 students were sampled from across 193 schools – but not all students were asked the same set of questions, for the HBSC section 29,063 were included. The survey was completed on computers and schools were encouraged to ensure privacy for the students.
Northern Ireland
Date: 2016
In Northern Ireland, there have been six rounds of the Young Persons’ Behaviour and Attitudes Survey (YBAS) (11-16-year-olds) since 2000, most recently in 2016. The most recent survey was of 6,831 children from 73 schools. Details of the survey can be found in the footnote [40].
Annex B: Factors that associate with underage drinking
Numerous studies have investigated the causes of underage drinking. Establishing causal factors is, however, challenging, as: many studies are necessary cross-sectional, which can identify associations but cannot prove causation; multiple factors will often associate together and therefore confound relationships; and the substantial differences in drinking culture makes using international studies difficult.
This section will prioritise those identified in systematic reviews and, where possible, draw on relevant cross-sectional data from the UK
In 2009, the Joseph Rowntree Foundation supported a large cross-sectional survey in England (Bremner et al.), which included a multiple regression analysis [41]. This enables the isolation of the strength of associations when controlled for confounding factors. NHS Digital performs a similar analysis on their recent 2018 data for England among current drinkers. The data from Scotland looks at a range of bivariant associations with current drinkers (ie relationships not controlled for confounding factors). These will all be discussed below as appropriate.
Sociodemographic factors
Age. Across all the parts of the UK, older children appeared to drink more frequently, and in the NHS Digital work it was the second strongest association with having drunk alcohol in the last week.
Socioeconomic status. In England, higher socio-economic status was correlated both with the probability of ever drinking and regular drinking [42]. Little difference is seen among Scottish 15-year-olds in regular drinking by deprivation [43], nor are there clear differences in Wales (figures not readily available for Northern Ireland) [44]. This was not found to be a strong association in the multiple regression analysis from Bremner et al.
Religion. Bremner et al. found that religion is associated with lower likelihood of ever having had a drink, which was particularly true of those identifying as Muslim.
Ethnicity. In England, White 15-year-olds were more likely to have ever drunk and drink regularly than their BME counterparts [45]. In Wales, the highest prevalence of regular drinking is seen in White Gypsy/Traveller, Caribbean or Black, and Arab backgrounds [46]. Ethnicity data not readily available for Scotland and Northern Ireland. NHS Digital identified White ethnicity as associating with drinking in the last week, and Bremner et al. found that White underage people were five times more likely than those with an Asian background to have drunk in the last week.
Gender. While there are small differences found between girls and boys in some parts of the UK on some measures, there does not seem to be a consistent robust impact of gender on underage drinking. This contrasts to drinking amongst adults. Bremner et al. found that, once other variables were controlled for, the only difference was in amount consumed, with boys more likely to consume higher volumes than girls.
Family factors
Yap et al. performed a large meta-analysis of 131 longitudinal studies to look for modifiable parental factors associated with initiation of drinking and levels of drinking [47]. They concluded that there was robust evidence for seven factors that were associated with initiation and drinking levels. These are discussed below, and where appropriate compared with cross-sectional work in the UK.
Parental provision of alcohol. This had the most robust relationship to both initiation and current levels of drinking. Adolescents whose parents make alcohol accessible for them to drink at home are both more likely to start drinking and to consumer higher quantities. This is controversial, with many people believing that exposure to alcohol early in the home is safer. The authors note that caution should be taken in applying this across cultures as alcohol socialization can differ substantially. However, this review found clear evidence to support policies against parental alcohol provision in cultures where tolerance of binge drinking is the norm.
Favourable parental attitudes towards young people drinking. As well as being identified by Yap et al., this factor had the strongest association to drinking in the last week in the analysis from NHS Digital.
Parental alcohol use. This has also been found in the cross-section studies in the UK, including the national statistic in England. Bremner et al. found that the association between observed parental drunkenness and initiation of drinking was stronger than that found with frequency of parental drinking. NHS Digital found that drinkers at home associated with drinking in the last week. It is worth noting that a 2016 systematic review concluded that while there was a consistent body of evidence for this association, differentiating it from confounding factors such as environmental, genetic, or cultural influences is difficult [48].
Parental monitoring. This is again reflected in the cross-sectional studies. In Scotland, children who reported higher parental knowledge of their activities were less likely be regular drinkers. In Bremner et al., once a range of factors were controlled for, the association between this and drinking initiation remained.
Parent-child relationship quality and parental support. These were identified as two distinct factors in the work from Yap et al. In the cross-sectional data, in Scotland, children who reported that they would talk to their family if they were really worried about something, were less likely to drink alcohol regularly.
Parental involvement. A series of cross-sectional studies in the US found that having regular family dinners strongly correlated with reduced substance use amongst teenagers, including alcohol [49]. In the work from Bremner et al., and in the data from Scotland, a greater number of evenings spent with friends (and thus fewer evenings spent at home) correlated with underage drinking.
Yap et al identified three more factors that were considered to have ‘emerging evidence’ as they were associated with initiation but only had equivocal associations with later levels of use. These were: rules against adolescent alcohol use; family conflict; and parental discipline more generally.
Peer factors
In England, as discussed above, if you ask children why they think their peers drink alcohol, the three top factors are peer-group related. Peer influence was also identified by Bremner et al. This should be approached cautiously however, as it is also possible that some, or even the majority, of this effect is due to peer selection (young people who are more likely to drink are more likely to choose friends who drink) rather than peer influence. Further, the interaction between families and peers is also complicated (ie families might be able to influence peers) [50].
Individual factors
Experience at school. A range of school-related experiences, such as enjoyment, school exclusion, post-school expectations, and truancy were associated with alcohol-use in the Scottish cross-sectional survey. In the NHS Digital analysis, playing truant associated with drinking the last week.
Emotional and behavioural problems. In Scotland, an association was found between experiencing mental and behavioural problems and drinking in the last week. The same was true on measures of mental wellbeing.
Mental wellbeing. In Scotland, lower mental wellbeing was associated with drinking in the past week.
Other health behaviours and experience. In the NHS Digital data for England, both recent drug use and smoking were associated with likelihood of having drunk in the past week. In Scotland, lower self-reported health was also associated with drinking.
Population level factors
The above has focused on factors that, within a given population, may influence the likelihood of one underage person drinking when another does not. However, as with adults, population-level factors are also important influences as to whether young people drink. The World Health Organisation identifies three ‘best buys’ as policies that have the greatest impact on alcohol harm, for the lowest cost, each of which are discussed briefly below [51].
Marketing. Exposure to alcohol marketing makes children more likely to start drinking and, if they are already drinking, to drink more [52]. A recent large study found that four in five young people (aged 11-19) had noticed alcohol marketing in the past month, with half of those aged 11-17 being exposed to 28 or more instances of alcohol marketing in that period [53]. For further information see our briefing on alcohol and marketing.
Price. This is a key policy, recommended by the WHO, as a way of reducing underage drinking [54]. For more information our briefings on the price of alcohol.
Availability. As it is illegal to purchase alcohol underage, access for children will often depend largely on the provision of alcohol by others (more on enforcement of age limits below). The work from the Joseph Rowntree foundation identified availability as one of the five key factors influencing underage drinking.
- Chief Medical Officer for England (2009). Guidance on the consumption of alcohol by children and young people.
- Government (accessed 20 May 2020). Alcohol and young people.
- World Health Organization (2018), Fact sheets: alcohol.
- Chief Medical Officer for England (2009). Guidance on the consumption of alcohol by children and young people.
- For the difference between alcohol-specific and alcohol-related hospital admissions see: The Institute of Alcohol Studies (accessed 19 June 2020). How alcohol mortality and morbidity rates are calculated in the UK.
- Public Health England (accessed 19 June 2020). Local alcohol profiles for England.
- Public Health England (accessed 19 June 2020). Local alcohol profiles for England.
- ScotPHO (accessed 19 June 2020). ScotPHO profiles.
- Public Health England (2016). Data intelligence summary: alcohol consumption and harm among under 18-year-olds.
- NHS Digital (2019). Smoking, drinking and drug use among young people in England 2018.
- Scottish Government (2019). Scottish schools adolescent lifestyle and substance use survey (SALSUS): alcohol report 2018.
- These results are presented in two different publications, by preference this work will use the second one. If the first is used it will be cited. Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A et al., editors. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe; 2020. Licence: CC BY-NC-SA 3.0; and Hewitt G., Anthony R., Moore G., Melendez-Torres G.J., Murphy S. (2019). Student Health and Wellbeing In Wales: Report of the 2017/18 Health Behaviour in School-aged Children Survey and School Health Research Network Student Health and Wellbeing Survey. Cardiff University, Cardiff, UK.
- Information Analysis Directorate (2017). Young persons’ behaviour and attitude survey 2016: health modules.
- Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A et al., editors. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe; 2020. Licence: CC BY-NC-SA 3.0
- NHS Digital (2019). Health Survey for England 2018: children’s health.
- Chief Medical Officer for England (2009). Guidance on the consumption of alcohol by children and young people.
- Public Health England (2016). Data intelligence summary: alcohol consumption and harm among under 18-year-olds.
- Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A et al., editors. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe; 2020. Licence: CC BY-NC-SA 3.0 IGO
- NHS Digital (2019). Smoking, drinking and drug use among young people in England 2018.
- The Institute of Alcohol Studies (2017). Like sugar for adults.
- The Institute of Alcohol Studies (2017). Like sugar for adults.
- Velleman, R. (2009). Influences on how children and young people learn about and behave towards alcohol: a review of the literature for the Joseph Rowntree Foundation (part one).
- World Health Organisation (2017). Tackling NCDs: “best buys” and other recommended interventions for the prevention and control of noncommunicable diseases.
- The Institute of Alcohol Studies, Alcohol and Marketing, factsheet (accessed November 2019)
- Critchlow, N. et al (2019). Awareness of alcohol marketing, ownership of alcohol branded merchandise, and the association with alcohol consumption, higher-risk drinking, and drinking susceptibility in adolescents and young adults: a cross-sectional survey in the UK. BMJ Open.
- WHO (accessed June 2020). Raising prices on alcohol through excise taxes and pricing policies.
- Oldham, M. et al. Youth drinking in decline. University of Sheffield, Wellcome Trust.
- Oldham, M. et al. Youth drinking in decline. University of Sheffield, Wellcome Trust.
- Oldham, M. et al. Youth drinking in decline. University of Sheffield, Wellcome Trust.
- NHS Digital (2019). Health survey for England 2018.
- Jivraj, S. (2012). How has ethnic diversity grown 1991-2001-2011? The University of Manchester, Joseph Rowntree Foundation.
- 2002-04 data from: NHS Health and Social Care Information Centre (2005). Smoking, drink and drug use among young people in England in 2004.
- RPIs from Office for National Statistics (accessed 19 June 2020). Inflation and price indices; 16-17 minimum wage from UK Government (accessed 19 June 2020). National minimum wage and national living wage rates.
- Pople, L. et al. (2014). The good childhood report 2014. The children’s Society.
- The Children’s Society (2019). The good childhood report 2019.
- NHS Digital (2019). Smoking, drinking and drug use among young people in England 2018.
- NHS Digital (2019). ‘Health Survey for England 2018’, Children’s health
- Scottish Government (2019). Scottish schools adolescent lifestyle and substance use survey (SALSUS): alcohol report 2018.
- These results are presented in two different publications, by preference this work will use the second one. If the first is used it will be cited. Inchley J, Currie D, Budisavljevic S, Torsheim T, Jåstad A, Cosma A et al., editors. Spotlight on adolescent health and well-being. Findings from the 2017/2018 Health Behaviour in School-aged Children (HBSC) survey in Europe and Canada. International report. Volume 2. Key data. Copenhagen: WHO Regional Office for Europe; 2020. Licence: CC BY-NC-SA 3.0; and Hewitt G., Anthony R., Moore G., Melendez-Torres G.J., Murphy S. (2019). Student Health and Wellbeing In Wales: Report of the 2017/18 Health Behaviour in School-aged Children Survey and School Health Research Network Student Health and Wellbeing Survey. Cardiff University, Cardiff, UK.
- Information Analysis Directorate (2017). Young persons’ behaviour and attitude survey 2016: health modules.
- Bremner P. et al. (2011). Young people, alcohol and influences: a study of young people and their relationship with alcohol.
- NHS Digital (2019). Smoking, drinking and drug use among young people in England 2018.
- Scottish Government (2019). Scottish schools adolescent lifestyle and substance use survey (SALSUS): alcohol report 2018.
- Hewitt G., Anthony R., Moore G., Melendez-Torres G.J., Murphy S. (2019) Student Health and Wellbeing In Wales: Report of the 2017/18 Health Behaviour in School-aged Children Survey and School Health Research Network Student Health and Wellbeing Survey. Cardiff University, Cardiff, UK.
- Ipsos MORI (2015). Health and wellbeing of 15 year olds in England: findings from the What about YOUth? Survey 2014. Health and Social Care Information Centre (now NHS Digital).
- Hewitt G., Anthony R., Moore G., Melendez-Torres G.J., Murphy S. (2019) Student Health and Wellbeing In Wales: Report of the 2017/18 Health Behaviour in School-aged Children Survey and School Health Research Network Student Health and Wellbeing Survey. Cardiff University, Cardiff, UK.
- Yap, M. et al. (2017). Modifiable parenting factors associated with adolescent alcohol misuse: a systematic review and meta-analysis of longitudinal studies. Addiction.
- Rossow I, Keating P, Felix L, McCambridge J. (2016) Does parental drinking influence children’s drinking? A systematic review of prospective cohort studies. Addiction.
- CASA (2012). The importance of family dinners VIII.
- Velleman, R. (2009). Influences on how children and young people learn about and behave towards alcohol: a review of the literature for the Joseph Rowntree Foundation (part one).
- World Health Organisation (2017). Tackling NCDs: “best buys” and other recommended interventions for the prevention and control of noncommunicable diseases
- The Institute of Alcohol Studies, Alcohol and Marketing, factsheet (accessed November 2019)
- Critchlow, N. et al. (2019). Awareness of alcohol marketing, ownership of alcohol branded merchandise, and the association with alcohol consumption, higher-risk drinking, and drinking susceptibility in adolescents and young adults: a cross-sectional survey in the UK. BMJ Open.
- World Health Organization (2017). Tackling NCDs: “best buys” and other recommended interventions for the prevention and control of noncommunicable diseases.
View this report