
In this month’s alert
Editorial – March 2015
Welcome to the March edition of Alcohol Alert, the Institute of Alcohol Studies newsletter, covering the latest updates on UK alcohol policy matters. In this issue, speculation surrounds the 2015 Budget; what will happen to alcohol duty? Other articles include: Lords join calls for a newer and more powerful EU Alcohol Strategy; and the Scottish football alcohol ban comes under pressure to be lifted.
Please click on the article titles to read them. We hope you enjoy this edition.
Budget 2015: NHS can’t afford cheap alcohol to become cheaper – but is anyone listening?
According to media reports, the Chancellor of the Exchequer will cave in to drinks industry pressure and lower beer duty in the 2015 Budget, a move that is seemingly supported by the Minister for Public Health Jane Ellison MP. It would be the third cut in as many years by George Osborne MP, who also announced the abolition of the alcohol duty escalator for wine and spirits last year.
Such a move would be another blow to public health campaigners, who argue that the National Health Service can’t afford for cheap alcohol to get cheaper. According to Treasury figures, tax cuts announced in last year’s Budget will lead to a loss of £1.5bn to the Exchequer over the next 5 years. This could fund the annual salaries of 9,571 nurses, 5.7 million hospital bed days, or over 1.3m emergency ambulance call-outs a year.
Chair of the Alcohol Health Alliance, Professor Sir Ian Gilmore, argued that a duty cut “lacked practical sense” and warned against the Treasury “throwing money away as a sop to the drinks industry”.
He said: “It [a cut in duty] seems to be sending all the wrong messages at a time when the NHS is under enormous strain, A&E departments are full to bursting point, when we know that price is the single biggest determinant of how much harm we see.”
Politicians put profit before Public Health
Calls to Drop the Duty have grown ever louder from the industry in the run-up to the annual Budget. The British Beer and Pub Association and Wine and Spirits Trade Association have led an intense lobbying campaign aimed at convincing MPs of the economic benefits of cutting alcohol excise duties. Industry representatives have met with Treasury officials and Cabinet figures including Exchequer Secretary Priti Patel MP and Chancellor Osborne himself, who hosted receptions on behalf of the All Party Parliamentary Group for Beer backing a beer duty cut. Members of the Alcohol Health Alliance have requested meetings with Patel and Osborne but have been unsuccessful.
AHA representatives have also been denied meetings with health ministers to discuss the potential impact of alcohol duty cuts on the NHS. Public Health Minister Jane Ellison MP did however find the time to lobby the Chancellor for a duty cut on behalf of alcohol industry trade bodies. In her response to Richard Siddle, editor of trade publication Harpers, she wrote: “I appreciate your concerns about the impact of alcohol duty and the need to stimulate economic growth… To share your views on a further cut, I have, as you ask, written to the Chancellor, enclosing a copy of your correspondence. I do hope that this is helpful.”
This move will likely generate great concern amongst health professionals. Simon Stevens, Chief Executive of NHS England called on the government to prioritise urgent action on cheap alcohol due to the enormous strain currently placed on A&E units. In an interview with the Telegraph, Stevens stated he wanted the NHS to ‘stand up and be counted’ in debates around alcohol pricing policies. With no apparent representations from health bodies made to the Chancellor, it looks likely that the profits of the drinks industry will triumph over public health once again in this year’s Budget.
Please follow our Soundcloud link to listen/download Professor Sir Ian Gilmore discussing the effects of lower duties on alcohol-related social and health harms.
Please read the Alcohol Health Alliance budget briefing paper Our NHS can’t afford for alcohol to get any cheaper for the facts behind the cost to the UK of further cuts to alcohol duty.
Pressure builds for a new EU Alcohol Strategy, but will it be enough?
The European Commission Committee on National Alcohol Policy and Action (CNAPA), which represents Member States, has called repeatedly for a new EU Alcohol Strategy to replace the former strategy, which expired in 2012. Since then, there have been numerous calls for it to be renewed including from public health bodies, NGOs, MEPs and, more recently, the UK House of Lords.
However, the nearest the Commission has come to agreeing to renew the strategy was to adopt, in 2014, an Action Plan on Youth Drinking and Heavy Episodic Drinking. CNAPA has said that this Action Plan “cannot be considered as a substitute to a new consolidated EU strategy to prevent and reduce alcohol-related harm” and reaffirmed the latter, being, in their view, a priority initiative.
CNAPA’s views are presented in a scoping paper to the European Commission. In the paper, CNAPA identifies a number of principles that should govern a comprehensive alcohol strategy:
- It should address all types of harmful use of alcohol and alcohol-related harm across all population groups
- It should be coherent and systematic, focused on both behavioural and structural prevention of alcohol harmful use
- It should reflect a ‘health in all policies’ approach, engaging the positive potential of all relevant policy sectors to help reduce harm from alcohol
- It should be evidence-based
- It should foster synergy across the global, European and national as well as regional and local levels, while respecting subsidiarity
The scoping paper emphasises the importance of actions at EU level in addressing cross-border issues, especially:
- EU rules on the mechanisms to influence prices (including alcohol taxation)
- EU definitions of alcoholic beverages that inhibit reduction of alcoholic content
- Alcohol marketing and advertising, including cross-border advertising and on-line advertising, with particular regard to the exposure of youth
- Labelling of alcohol products
Mariann Skar, Secretary General of Eurocare, the European Alcohol Policy Alliance, warmly welcomed the scoping paper from the Member States. She said: “We now expect the European Commission to be quick and follow up the Member States’ request for increased action on preventing and reducing alcohol-related harm. As the scoping paper explains, there are several issues which need to be addressed at EU level, such as advertisement and information to consumers, and it is important that the European Commission includes the recommendations from the Member States in their future work.”
However, the prospects are uncertain for a renewal of a fully comprehensive alcohol strategy at EU level. The pressure for renewal from within the Commission appears to have diminished and there has always been opposition to a strategy from non-health stakeholders and sectors of the alcohol industry. The European Parliament Committee for Environment, Food Safety and Public Health is currently considering a resolution for the adoption of a new EU Alcohol Strategy to be presented to the European Parliament. However, public health bodies and NGOs have written to MEPs expressing their concerns that suggested amendments to the resolution appear to prioritise commercial interests over public health.
Lords call for a new EU Alcohol Strategy with effective legislation at Commission level
A report published by the House of Lords EU Committee supports the European Union acting in its own power to combat alcohol-related harm. A New EU Alcohol Strategy? argues that any new action by the EU should focus on measures within its powers, and not rely just on action by Member States, or voluntary commitments from industry.
The report reaches three main conclusions from its inquiry into the previous strategy:
- The 2006-12 strategy, while well-intentioned, did not concentrate on what the EU itself can act on. Consequently it achieved little. In developing any new action the EU should therefore concentrate on what it can do, over and above any initiatives the Member States can take on their own. In particular, the EU should ensure that its own policies contribute to the reduction of alcohol-related harm and excessive drinking.
- The current EU alcohol taxation regime prevents Member States from raising duties on the most harmful substances, and provides incentives to purchase drinks with higher alcohol contents. This illogical taxation structure must be reformed.
- The EU rules on food labelling must be amended to include alcoholic drinks. These labels should include, as a minimum, the strength, the calorie content, guidelines on safe drinking levels, and a warning about the dangers of drinking when pregnant. Voluntary commitments are not enough.
Committee Chair, Baroness Prashar, said that the inquiry identified the need for the EU to conduct more satisfactory cross-border research on alcohol abuse, its effects, and what works to prevent it. The inquiry also suggested that the UK Government “should honour the commitment it gave in 2012” by introducing minimum unit pricing if it proved successful in bringing health benefits to the heaviest drinkers in Scotland.
Responding to the report, Katherine Brown, Director of the Institute of Alcohol Studies said:
“We welcome the recommendations made by the House of Lords. They provide some much needed common sense at a time when the EU Alcohol Strategy appears to be the victim of bureaucratic blunders in Brussels. With alcohol use the third leading cause of death and disability in Europe, the absence of a comprehensive policy to tackle this issue is indefensible.
“The European Commission has repeatedly ignored calls from Member States and public health professionals for a new EU Alcohol Strategy. We cannot afford any further delays, so let’s hope that this report provides impetus for action.”
A new EU alcohol strategy? was published by the EU Sub-Committee on Home Affairs, Health and Education.
CMA clarifies position over super-strength alcohol schemes
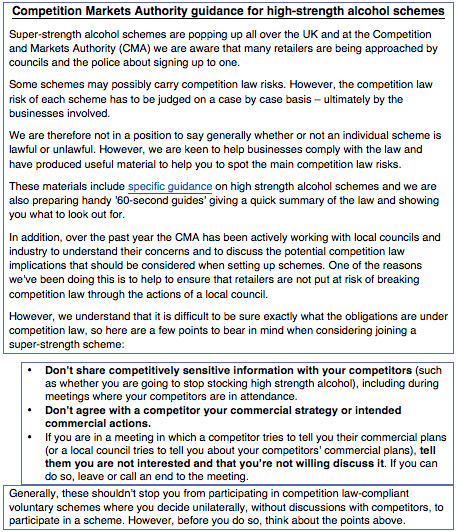
The Competition Markets Authority (CMA) has produced a statement in the wake of the press coverage of the meeting held by the All Parliamentary Party Group for Beer in January. Then, Dan Moore, Director of Competition and Markets at the CMA, spoke about the potential for some schemes to carry competition law risks. This was interpreted in an Off Licence News article as an admission of knowledge that some local authorities had breached competition law in promoting the schemes.
The CMA has since declared its position in its guidance to organisations (see below). This indicates clearly that the CMA is not able to say whether or not an individual scheme is lawful or unlawful.
As the Local Government Association states, Reducing the Strength refers to initiatives designed to tackle the problems associated with street drinking by removing from sale low price high-strength alcohol products through voluntary agreements with local retailers. Suffolk was the first area to adopt the approach back in 2012 and since then a number of other places have followed.
The models used vary from place-to-place, but tend to target alcohol products above 6.5% alcohol by volume (ABV), although some have focused on a slightly lower ABV or lower cost products.
The LGA commented: “Over the last fifteen months, the Competition and Markets Authority (CMA) have provided clear and consistent guidance on the competition law risks associated with Reducing the Strength schemes. The LGA worked with the CMA, councils and industry / retail associations over several months to develop best practice guidance for councils that are considering introducing Reducing the Strength schemes. The guidance was published at the end of 2014, and we are continuing to work with the CMA to ensure it is kept up to date and reflects best practice.”
Pressure mounts to lift Scottish alcohol football ban

A campaign to lift the ban on sales of alcohol at football grounds in Scotland is gaining momentum. The Scottish Labour Party is leading the campaign, with the Scottish Conservative Party and the Scottish Football Association (SFA) also in support. The SFA is seeking the views of fans on whether alcohol should be sold at stadiums during matches, and it has said it wants to “build a case” in favour of lifting the ban. However, the Scottish police have expressed reservations, and the Scottish National Party Government has said it has no plans to end the ban, initially imposed following a riot at the 1980 Scottish Cup final between Rangers and Celtic.
However, alcohol can be served in corporate hospitality areas of football stadiums.
Jim Murphy, leader of the Scottish Labour Party, has attacked the ban as being a form of class prejudice. He said that football supporters should not be treated differently from rugby fans at Murrayfield, where drinking is permitted.
Mr Murphy, a Celtic fan who is himself teetotal, said: “We know there has been a problem in the past but this group of supporters shouldn’t have to pay for the mistakes of their grandfather’s generation… I think we should stop criminalising football fans and stop treating them as uniquely incapable of drinking in moderation and enjoying a sporting occasion. It’s about treating football fans as adults and done properly, it can improve the experience of the stands.” But Mr Murphy added that ending the ban “shouldn’t be driven by a desire of football clubs to boost their income or fleece supporters.”
However, there is not a complete consensus on the issue. The head of Police Scotland, Chief Constable Sir Stephen House, has said he would be “extremely concerned by any proposal to amend legislation in respect of alcohol at football matches in Scotland”. But, he said, if the outcome of an independent public consultation backed the idea, then “we will of course enter into formal discussions with the footballing authorities.”
Social Justice Secretary Alex Neil told BBC Scotland that reintroducing the sale of alcohol would threaten the game’s status as a “family event” and could lead to a rise in football-related domestic violence.
He said: ” We don’t believe now is the right time to reintroduce alcohol into football. The fact is that when we were selling alcohol at football matches there were many more problems in terms of crowd behaviour than there are today.
“We have made a lot of progress so let’s not turn the clock back. Let’s keep with that progress, keep it a family game and if people then want to go for a drink after the game then they are free to do so.”
Scottish Health Secretary Shona Robison also criticised the campaign. She said:
“Scotland has a difficult relationship with alcohol and our position has been to reduce alcohol consumption. I just think this goes in completely the wrong direction.
“I am not convinced we have seen the eradication of football-related violence. In fact I think we see it still far too much.”
Public health organisations voiced their concerns over lifting the ban in a letter to the Herald Scotland newspaper. The signatories – which included SHAAP, BMA Scotland, and Alcohol Focus Scotland – also expressed their disappointment at not being involved in the consultations taking place over the issue.
Alcohol ban to be introduced on railway trains?
There is uncertainty in regard to whether or not the rail safety authorities are considering banning the drinking of alcohol on trains to prevent the deaths of drunken passengers. The measure is mooted by the rail safety watchdog, the Rail Safety and Standards Board, in a Platform Train Interface Strategy reviewing the whole issue of passenger safety in relation to stations, platforms and getting on and disembarking from trains, and behaviour on trains. However, spokesmen for the Board later denied that there was intention of introducing an alcohol ban.
Drunkenness factor in two-thirds of incidents
The review states that 48% of the passenger-fatality risk on the rail network happens when passengers are getting on or off trains, and in 21 of the 32 such deaths in the past 10 years, drunkenness was a factor. Intoxication is associated with the potential for passengers to fall from the platform, be struck by a train while on the platform, fall between the platform and the train or slip, trip, or fall across the platform train interface. Men are involved in more alcohol-related incidents than females, the review explains. Altogether, intoxication is stated to be the fourth biggest incident factor by number of incidents and a feature of 9% of all incidents.
The strategy review contains a section titled ‘Advancing the management of intoxicated passengers’. This says that to support the management of intoxicated passengers, the feasibility and effectiveness of enhancing station facilities (informed by good practice) will be assessed, along with the potential to advance co-ordinated support between station staff, train staff, Network Rail, and the British Transport Police (BTP) to improve implementation of existing legislation and promote “responsible drinking” on the railway.
Based on the work achieved in the immediate term, consideration will be given to the development of additional good practice on the management of intoxicated passengers, which will include guidance to staff on how to apply it.
The alcohol ban
In terms of the strategic response to intoxicated passengers, the review states that a range of resources to support the safe management of intoxicated passengers will be piloted at all staffed stations and, where successful, will be implemented across the network. Work will also be undertaken to incorporate requirements for such resources into the design standards for new stations. The exploration of potential advancements in co-ordinated support between station staff, train staff, Network Rail, and the BTP will be turned into formalised agreements of roles, responsibilities, and processes for managing intoxicated passengers. This formalised agreement will be supported by investigation into additional legislation and policy that could be used to support the management of intoxicated passengers; for example, banning the sale and consumption of alcohol on trains, similar to the ban already in operation by Transport for London (TFL) in relation to buses and underground trains.
However, spokesmen for the Board later insisted that the idea of a similar alcohol ban on the railways was totally wrong, and that the strategy document was referring only to existing bans and by-laws, such as the Scottish ban on alcohol consumption on night-time train services and the localised restrictions on some trains carrying football supporters.
Tube strike called over failed alcohol breath test
A strike has been called on the London Underground in protest at the sacking of a tube train driver who twice failed an alcohol breath test before starting work on the Northern Line. Union officials insisted that the driver was not drunk and had not been drinking at work and that the positive breath test was due to the driver suffering from diabetes. However, London Underground said the breath tests were unaffected by diabetes and the case had gone through a full disciplinary hearing and appeals process, as well as a separate independent director’s review.
As reported by the BBC, the transport authority said it had explored in detail the suggestion that diabetes could affect the breathalyser result, but concluded that the type of test it used was not affected by acetone, which is produced in the bloodstream of people with the condition.
However, Mick Cash, General Secretary of the Rail, Maritime and Transport (RMT) Union which has called the strike, said there had been a campaign of “misinformation and smears” against his organisation.
He said: “This action is the first stage as part of a rolling programme of industrial action and I urge all RMT London Underground train operators and instructor operators to stand firm together against this and any future injustices against RMT members.”
Nick Brown, Chief Operating Officer of London Underground (LU), said: “This indefensible strike is about one RMT member dismissed for failing two alcohol breath tests. We will not be swayed by it as we will never compromise on the safety of our customers and staff. You wouldn’t let someone who had been drinking alcohol drive your family in a car, and we don’t let people who have been drinking alcohol drive people’s families in Tube trains.
“For the RMT leadership to announce a strike regardless shows how completely out of touch they are, just as the timing demonstrates that they know they have very little support from their members on this issue.”
Members voted by 299 votes to 221 to take action. The turnout was 42%. LU said the number of drivers who had voted to take strike action represented 8% of all drivers.
In December, RMT workers held a 24-hour strike on the Northern line over the same issue.
UK alcohol deaths still above 1990s levels
Office for National Statistics (ONS) data show a small increase in the number of alcohol-related deaths compared with the previous year. In 2013, there were 8,416 alcohol-related deaths registered in the UK, 49 more than in 2012, when there were 8,367 deaths. The age-standardised rate remained the same (14.0 deaths per 100,000 population).
Alcohol-related Deaths in the United Kingdom, Registered in 2013 provides a relatively conservative estimate for the number of alcohol-related deaths in the UK. An updated method for estimating the impact of alcohol on population health by researchers at the Centre for Public Health, Liverpool John Moores University, found that in England over 21,000 deaths were caused by alcohol consumption in 2010.
Longer-term trends show that the alcohol-related age-standardised death rate has fallen in recent years. However, it remains significantly higher than 20 years ago, when there were 9.1 alcohol-related deaths per 100,000 population (illustrated below).
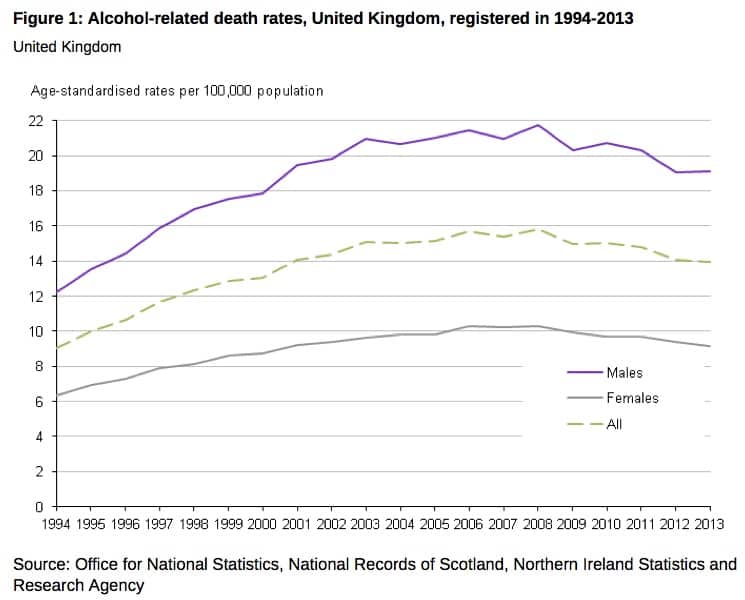
Death rates have remained relatively stable for the past ten years following a large increase during the previous decade. Between 2003–2013 alcohol-related death rates fell from 15 to 14 per 100,000 population; however, between 1994–2003 these rates had risen from 9 to 15 per 100,000.
For both sexes, UK alcohol-related death rates were highest among those aged 60 – 64 years (45.3 deaths per 100,000 males and 22.4 per 100,000 females), alcoholic liver disease being the most common cause. Among that age group, the number of deaths from alcoholic liver disease alone in England and Wales has increased by over 50% since 2003. However, importantly, these statistics show that 43% of alcohol-related deaths amongst men and 41% amongst females occur among those aged under 55, indicating that alcohol-related ill health is a major burden on adults of working age.
Does your occupation matter?
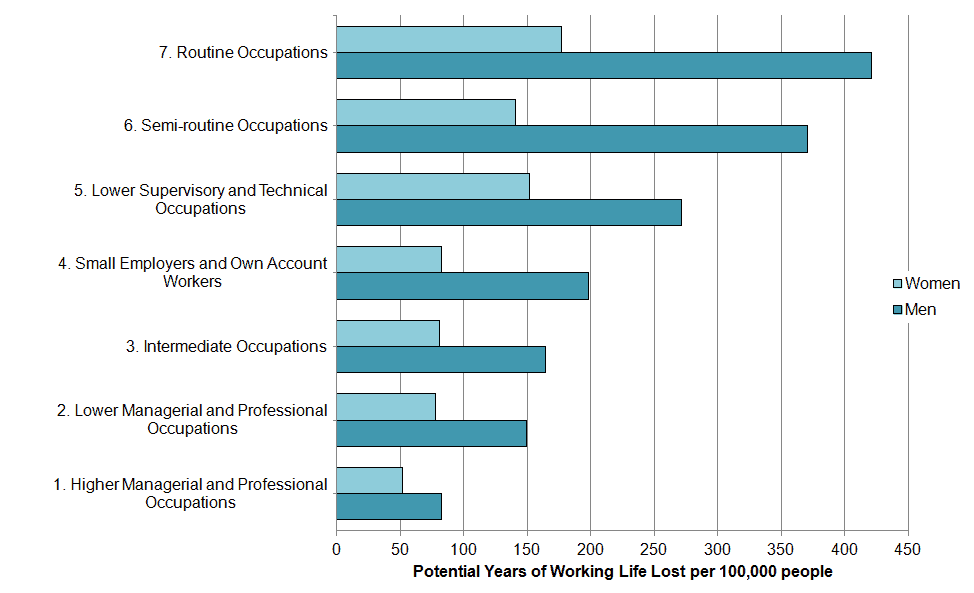
The ONS produced an accompanying report examining the socio-economic and gender inequalities in alcohol-related deaths among working age adults. The analysis showed that those in routine occupations tended to have higher death rates and lose more potential years of working life because of alcohol-related deaths than those in more advantaged socio-economic classes.
Using the 2011 Census data, the ONS found that alcohol-related death rates for those in routine occupations (e.g. bar staff, cleaners and labourers, with 29.5 deaths per 100,000 men and 12.6 deaths per 100,000 women) were four times greater for men and two times greater for women, than those in professional roles (e.g. doctors, IT strategy and planning professionals and lawyers, with 7.3 deaths and 5.2 deaths per 100,000 men and women respectively).
In 2011, the largest significant gender difference was found in semi-routine occupations (e.g. veterinary nurses, traffic wardens and security guards), where the rate was almost three times greater for men than women. In contrast, the higher managerial and professional occupations were the only class without a significant gender difference in the alcohol-related death rates (Alcohol-related death rates by occupation, illustrated).
The ONS figures add to the established body of evidence indicating that there is an inverse relationship between socioeconomic status and alcohol-related harms, despite people from higher income groups drinking more. The Institute of Alcohol Studies 2014 report Alcohol, Health Inequalities and the Harm Paradox evaluated the evidence base, concluding that the poorer health of lower socioeconomic groups was more likely to be linked to alcohol’s interaction with other unhealthy behaviours.
Drink-drive fatalities up a fifth
Provisional estimates from a new release by the Department for Transport indicate that between 230 and 290 people (central estimate 260) were killed in drink-drive accidents in Great Britain. Drink-drive deaths now account for around 15% of all road fatalities.
There were also an estimated 250 fatal drink-drive accidents in 2013, an increase of 19% (40) on 2012 (210). If this figure is confirmed in the final figures later this year, it will be the highest number of fatal drink-drive accidents since 2009.
In contrast, the total number of drink-drive accidents of all severities fell by 14% to 5,710 in 2013. This means that around 4% of all reported road traffic accidents in 2013 involved at least one driver over the drink limit. It is also the lowest number of drink-drive accidents on record.
Men are more likely to drink and drive than women. In 2013/14, 8.1% of men admitted to driving when over the limit at least once. In comparison, 3.5% of women admitted to the same offence.
Young drivers most likely to be “under the influence”
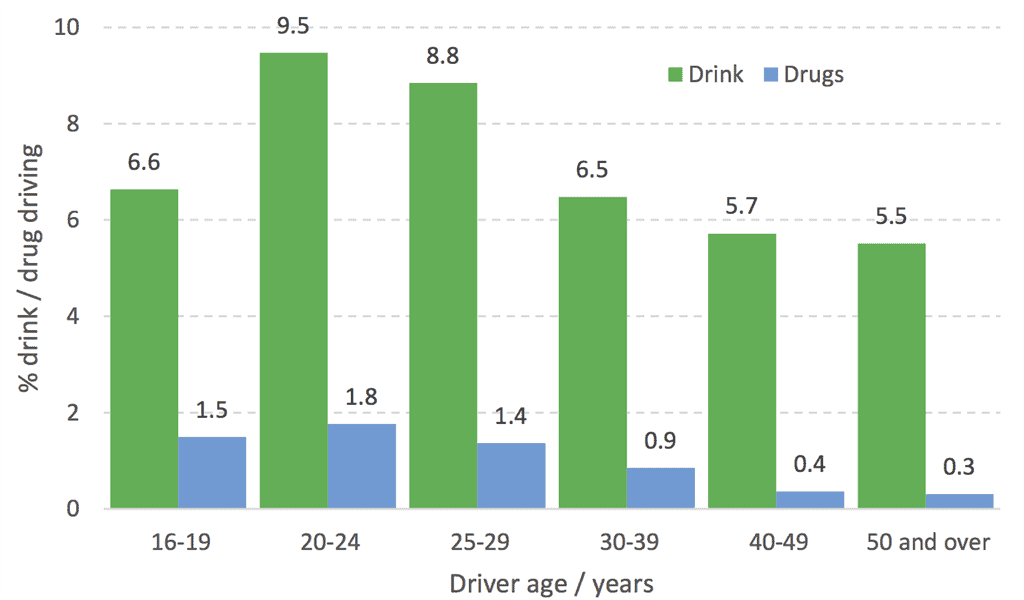
In 2013/14, 5.9% of drivers admitted to driving when they thought that they might have been over the drink-drive limit. Self-reporting figures also revealed drink-driving problems among young drivers, with nearly a tenth (9.1%) of drivers in their 20s admitting to drink-driving compared with around 5.6% of drivers aged 40 or older (see illustration).
These figures indicate that driving under the influence of alcohol or drugs is mostly a problem in younger, rather than older, drivers. However, continuous monitoring of the figures will be required to assess whether the problem remains in the cohorts (i.e. whether young drivers who offend today continue to offend when they get into the older age groups) or whether it is an age-related problem (i.e. whilst drivers offend at younger ages, they then stop offending as they get older).
Historically, figures showing the number of drink-drive fatalities in drink-drive accidents today are more than six times lower than in 1979, when records began. The total number of drink-drive casualties has fallen by 74% since.
Drink-drive ‘loophole’ to be closed
The legal provision allowing motorists suspected of drink-driving offences to demand a blood or urine test after having provided a positive breath test at the roadside is to be rescinded by the Deregulation Act now going through Parliament. The reform is expected to come into force in April 2015.
The move is in response to ministerial concerns that many drivers are attempting to buy time to sober up by asking for a blood or urine sample to be taken by a doctor. This takes place at a police station and there can be a delay of some hours before the additional tests are carried out. Currently, the results of the blood or urine test replace those of the roadside breath test.
The bill also requires convicted drink-drivers to take medical tests to prove that they are not alcohol-dependent before being allowed to drive.
The official impact assessment of the measure states that the blood/urine test option “is a redundant provision, which uses significant resources”. It states that the overall policy aim is to contribute to streamlining the enforcement process for drink-driving to ensure the more efficient use of police resources; to make the application of the drink-driving law fairer to suspects, regardless of how they are tested and their knowledge of the law; to ensure that people who are driving above the prescribed limits for drink are prosecuted successfully; to increase the efficiency and effectiveness of enforcement activity using current equipment; to increase the efficiency and effectiveness of enforcement activity using mobile evidential breath testing equipment; and to contribute towards more credible and effective drink-driving law.
Additionally, police will have more powers to prosecute suspected drug-drivers – motorists under the influence of illegal substances or high levels of prescribed drugs.
Edmund King, president of the Automobile Association (the AA), supported the move. He said that tightening the legislation around alcohol testing would “help close the loopholes that some drivers exploit to play for time when they know they have drunk close to the limit. Our advice to drivers remains constant: if you are going to drive then don’t drink and if you are going to drink then don’t drive.”
However, the UK Government has so far declined the opportunity to reduce the permitted blood alcohol level for drivers to the level applying in almost all other European Union countries, despite Scotland doing so at the end of last year (2014).
Rise of the young teetotaller
The drinking habits of young people are behind the lower consumption levels among Britons today compared with a decade ago, according to the Office for National Statistics (ONS).
The Adult Drinking Habits in Great Britain survey shows that more than a fifth (21%) of adults have now cut alcohol from their diets. The ONS named a fall in binge drinking levels since 2005 and a rise in the proportion of 16 to 24-year-olds going teetotal as influential factors behind the changes in consumption.
Binge drinking – defined as exceeding eight units of alcohol on their heaviest drinking day in the week for men and six units for women, and 2-3 units for women – fell from 18% to 15%, although there has been little change since 2011. This was partly because fewer adults chose to drink alcohol and partly because when people did drink they consumed less”, said the ONS.
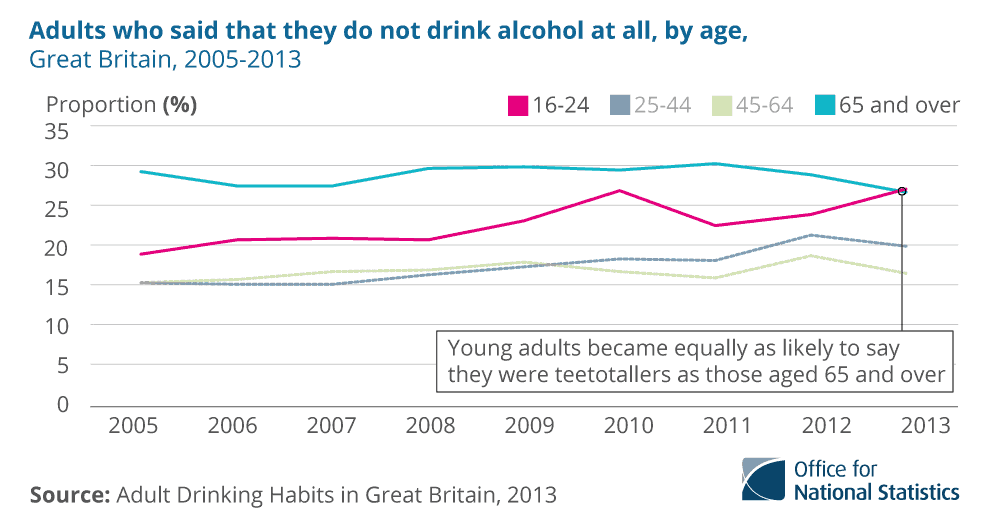
The report also stated that the falls in drinking between 2005 and 2013 “were a result of changes among younger adults, with little or no change in older groups”. This was demonstrated by the 40% rise in the proportion of teetotal 16 to 24-year-olds over the period. This age group is now just as likely to abstain from alcohol as those aged 65 and over (27%; illustrated below).
Young adults are also mainly responsible for the fall in binge drinking since 2005; the proportion that had binged decreased by more than a third from 29% to 18% in 2013. However, those who did drink remained the most likely group to have binged. Although far lower, the proportion of those aged 65 and over who binge drink is on the rise again (illustrated below).

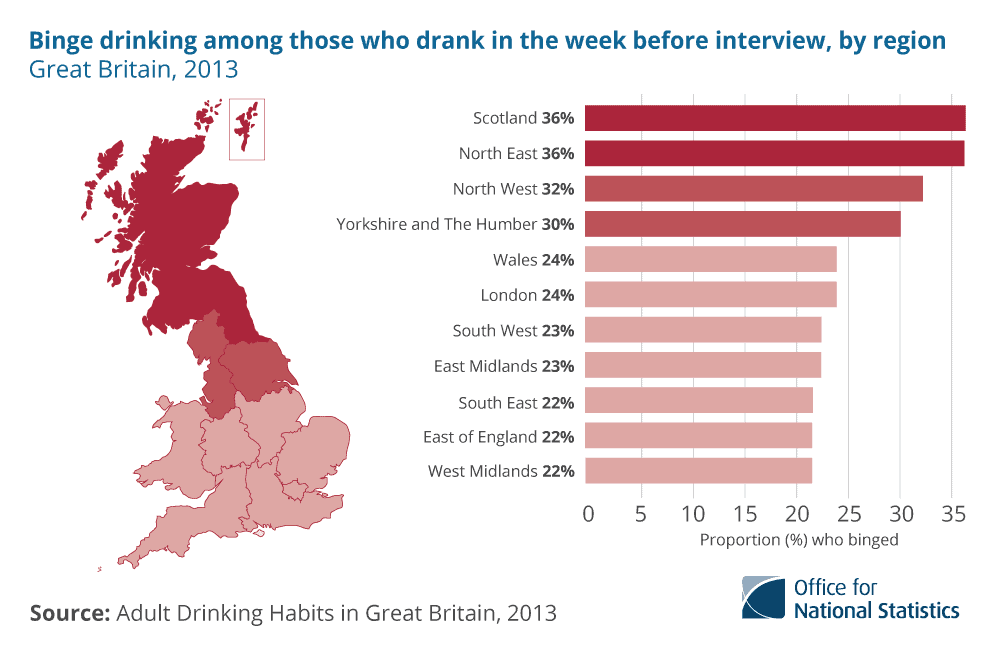
Almost a third of adults in London (32%) said that they do not drink alcohol, considerably more than anywhere else in Great Britain. By contrast, adults in the North East of England and in Scotland who drank in the last week were more likely to have binged than other Britons (36%).
Responding to the data, Professor Sir Ian Gilmore, Chair of the Alcohol Health Alliance UK said:
“These results today are an encouraging sign; however, there is absolutely no room for complacency. Whilst the average level of consumption has fallen, this may be, in part, due to the change in the ethnic makeup of the country, with many people abstaining from drinking altogether. Data on alcohol consumption is also unreliable; many people under-report how much they drink and self-reported data on consumption does not correlate with sales data.
“Enough alcohol is sold in the UK for all consumers to be drinking above the low risk guidelines. Alcohol remains the biggest single cause of death in under-60s in the UK and globally, more alarmingly, people are dying at a far younger age.
“The overall numbers of alcohol-related deaths may be down but the numbers are still far higher than they were twenty years ago. Without effective action from Government on pricing, marketing and availability, we are storing up major problems for the future.”
34,000 alcohol-related hospital admissions cost Welsh NHS £109m a year
The Welsh government is to work to improve the country’s response to alcohol harm with a specific aim being to reduce the negative impact on the health service. Deputy Health Minister Vaughan Gething revealed figures showing that there are 34,000 hospital admissions caused by alcohol misuse every year costing the Welsh NHS £109m annually.
Speaking at a conference about alcohol-related brain damage, the Deputy Minister said that figures show 42% of adults in Wales report drinking more than the recommended guideline amount of alcohol at least once in the last week. New statistics for alcohol-related deaths show there were 467 deaths in Wales in 2013.
The Public Health Observatory report Alcohol and Health in Wales 2014 revealed that in 2012-13 there were around 21,700 males and 12,300 females admitted to hospitals in Wales with alcohol-attributable conditions.
The Deputy Minister confirmed that the Welsh Government will invest almost £50m in 2015-16 in initiatives to tackle the harms associated with both alcohol and drug misuse.
The investment made since the Welsh Government’s substance misuse strategy, Working Together to Reduce Harm, was launched in 2008 has enabled significant progress to be made.
There has been clear progress on reducing waiting times for treatment, with the percentage of clients starting treatment within 20 working days increasing from 73% in 2009-10 to 87% in 2013-14, continuing the trend of improvement over the five-year period.
 Mr Gething said:
Mr Gething said:
“Alcohol misuse is leading to a range of well-evidenced health and social harms, particularly for the significant minority of people who drink to excess and do not recognise the harm they are doing to themselves and others.
“While there has been an overall downward decline in the number of alcohol-related deaths in Wales since 2008, that people die as a result of consuming too much alcohol is still a stark reminder of the challenges we still face in tackling the causes and impact of substance misuse.
“Each of these deaths is a personal tragedy for the individuals and their family and friends and illustrates the importance of having good-quality, responsive local alcohol treatment services.
“Since 2008, there has been general reduction in waiting times for both assessment and treatment. Today’s conference on alcohol-related brain damage is also important so that we can improve diagnosis and continue to develop evidence-based treatment responses to the implications of excessive alcohol misuse.
“I am determined that we must not be complacent and we must explore the use of all the policy levers available to us to tackle and reduce the harms that substance misuse causes to society as a whole.”
Alongside a range of education and prevention initiatives, the Welsh Government is also currently taking forward the preparatory work necessary to introduce a minimum unit price for alcohol in Wales.
Home Office decides against locally set licensing fees
Licensing fees have been contentious ever since the introduction of the 2003 Licensing Act, which failed to address the issue adequately. Last year’s consultation on the issue came after continued pressure, but was criticised for its narrow scope. Now, after a 10-month wait, the Home Office has formally responded to the consultation, but the wait for answers and effective action continues.
 Lynne Featherstone MP, Minister of State for Crime Prevention, announced that the government would not proceed with locally set fees, but that they did want further evidence from the LGA on the issue. She stated that: “Fee payers were strongly opposed to locally-set fees and concerned that fees would rise significantly without justification. Many were particularly critical of the evidence base.”
Lynne Featherstone MP, Minister of State for Crime Prevention, announced that the government would not proceed with locally set fees, but that they did want further evidence from the LGA on the issue. She stated that: “Fee payers were strongly opposed to locally-set fees and concerned that fees would rise significantly without justification. Many were particularly critical of the evidence base.”
However, the LGA described the decision as ‘hugely disappointing’ given the fact that many councils are currently unable to cover their costs using the nationally set licensing fee system, having instead to subsidise the licensed trade to significant amounts.
Responding for the LGA, Cllr Ann Lucas OBE, chair of the LGA’s Safer and Stronger Communities Board, said the licensed trade had benefited from around £170m of taxpayers’ money in the past decade. “At a time when every penny is needed to protect services, this money would help patch up our crumbling roads and ease the pressure on squeezed social care budgets,” she said. “The Home Office has accepted the principle of locally-set licensing fees by introducing them as part of the recent Scrap Metal Dealers Act. It makes little sense to then decide they can’t be introduced for the Licensing Act.”
As part of the consultation, the Government had asked local authorities to provide evidence of their licensing costs. However, only a small number responded to this, and as a result the Home Office described the information it received as providing only a “limited and contradictory picture of the relationship between licensing authority costs and income.” As a result it was “not in a position to determine the details of the proposed new fees regime or predict its consequences with confidence,” and so have invited the LGA to provide better evidence of licensing authorities’ costs.
On-going research into the licensing system by IAS has identified a range of views from local authorities on the issue of locally set fees. Not all authorities are in favour, although all agree that there is a pressing need to ensure that licensing costs can be fully recovered via fees.
Hidden harm: Alcohol’s devastating impact on children and families
 A new study has revealed the full extent of alcohol-related family and domestic violence in Australia. More than one million children are estimated to be affected in some way by others drinking, 140,000 are substantially affected and more than 10,000 are in the child protection system because of a carer’s drinking.
A new study has revealed the full extent of alcohol-related family and domestic violence in Australia. More than one million children are estimated to be affected in some way by others drinking, 140,000 are substantially affected and more than 10,000 are in the child protection system because of a carer’s drinking.
The new study was officially launched at New South Wales Parliament House by Rosie Batty, family violence campaigner and 2015 Australian of the Year. Funded by the Foundation for Alcohol Research and Education (FARE) and undertaken by the Centre for Alcohol Policy Research (CAPR), the study, ‘The hidden harm: Alcohol’s impact on children and families’, examined the prevalence and effects of heavy drinking on families and children and the extent to which they persisted or changed over time.
The study is a further example of the increasing attention being paid internationally to the adverse effects of alcohol on people other than the drinkers themselves, particularly family members and children, the phenomenon sometimes referred to as ‘passive drinking’. In 1998, The Institute of Alcohol Studies, in association with Eurocare, prepared for the European Commission a report on alcohol and harm to families in the European Union, and in the UK there have been a large number of subsequent reports on the subject, and some political action, with improvements being made to the national response to family members damaged by the harmful drinking of another, normally a parent. In 2011, in furtherance of a commitment by the Coalition Government, the National Treatment Agency for Substance Misuse in England issued guidance to improve service provision:’Supporting information for the development of joint local protocols between drug and alcohol partnerships, children and family services‘, and a pioneering alcohol and drug family court had already been established in 2008.
Australian findings
The Australian study found that, in 2011, there were almost 30,000 police-reported incidents of alcohol-related domestic violence in just the States and Territories where such data is available, with the figure excluding alcohol-related assaults in Queensland, South Australia, Tasmania and the Australian Capital Territory.
The new study draws on two national surveys of alcohol’s harm to others, service system data from policy and child protection services and information gained from qualitative interviews with families affected by others’ drinking, which revealed that children experienced a range of harms.
The harms reported by families varied. Children were verbally abused, left unsupervised, physically hurt or exposed to domestic violence as a result of others’ drinking. Most commonly, children witnessed verbal or physical conflict or inappropriate behaviour.
More than one quarter of respondents reported harm from the drinking of family members in at least one of the surveys undertaken in 2008 and 2011. These harms often persisted over time, with 50% of adult respondents harmed in 2008 also harmed in 2011 and 35% of children harmed in 2008 also harmed in 2011.
The study follows the release of the report ‘The Range and Magnitude of Alcohol’s Harm to Others‘ (2010), which was the first Australian study to examine the harms from alcohol consumption on people other than the drinker.
With approximately half of reported domestic violence incidents and up to 47% of child protection cases involving alcohol, FARE Chief Executive Michael Thorn said the need was to understand alcohol’s role in family and domestic violence and use this information to act to prevent this violence from occurring.
FARE has developed a policy options paper, in consultation with public health, domestic violence and family services, to propose a framework for action to prevent and reduce alcohol-related family and domestic violence. The policy options paper proposes a range of measures which can be implemented across the community, that focus on preventing violence before it happens, intervening early to prevent further harms for victims of violence and ensuring that service responses are appropriate. Mr Thorn said there was no one single solution to reduce alcohol-related family violence.
“If we are serious about reducing alcohol-related family violence, we have to consider a wider range of policy measures,” he said. “We need national public education campaigns that acknowledge and address the role of alcohol in family violence; we need targeted screening of young people at greater risk of harm; and measures that reduce the availability, target the price, and regulate the promotion of alcohol; together with efforts to improve the way in which the alcohol and other drugs sector collaborates with domestic violence, child protection and mental health services.”
Family Drug and Alcohol Courts to be extended in England
Special courts set up to help parents with drug or alcohol addiction overcome their problems so that they can keep their children are to be opened in more areas of England. The expansion is being funded by a £2.5 million grant from the Department for Education.
A pioneering Family Drug and Alcohol Court (FDAC) was opened in London in 2008, and courts have opened more recently in Gloucestershire and Milton Keynes. More will now open in areas including East Sussex, Kent and Medway, Plymouth, Torbay and Exeter, and West Yorkshire.
The majority of families which come into care proceedings have at least one parent with a drink or drug problem thought to be causing harm to the children. Unlike conventional care proceedings, parents in FDAC see the same judge throughout and meet with them every fortnight. They also receive support from a multi-disciplinary team, which helps them access substance misuse services and provides assistance in tackling other problems such as housing, domestic violence and financial hardship.
They undergo regular testing to make sure they are not secretly drinking or taking drugs.
The Nuffield Foundation funded Brunel University to carry out an independent evaluation of the pilot Family Drug and Alcohol Court. This ran from January 2008 to March 2012 at the Inner London Family Proceedings Court. The multi-disciplinary team was provided by the Tavistock and Portman NHS Foundation Trust, in partnership with children’s charity, Coram. The pilot was based on a successful US model and began with three participating London Boroughs – Camden, Islington and Westminster. Hammersmith and Fulham and Southwark joined the pilot in 2012.
The main findings of the evaluation were that the pilot was successful in achieving its objectives:
- FDAC families had higher rates of substance misuse cessation than those who had been through ordinary care proceedings: 40% of FDAC mothers compared to 25% of comparison mothers, and 25% of FDAC fathers compared to 5% of comparison fathers, although the data on fathers was less complete than for mothers
- FDAC families had higher rates of family reunification: 35% of FDAC mothers stopped misusing and were reunited with their children, compared to 19% of mothers who had been through ordinary care proceedings
- The rate of neglect or abuse one year after children returned home was lower for FDAC parents than parents who had been through ordinary care proceedings: 25% compared to 56%
- In cases where reunification was not possible, FDAC was no quicker in achieving alternative permanent placement than ordinary proceedings (62 weeks)
- In addition to receiving the intensive service from the FDAC team, a higher proportion of FDAC mothers (95% v 55%) and fathers (58% v 27%) were offered help from other agencies for their substance misuse.
The success of the FDAC has been widely acknowledged, notably by Sir James Munby, president of the Family Division of the High Court.
He said: “I consider FDAC as one of the most important and innovative developments in public family law in decades. (The FDAC model) appeals to both the heart and to the head. It is a mix of compassion, firmness and clear-eyed assessment of the parent’s realistic chances of achieving rehabilitation. The process delivers better outcomes for the children and the parents subject to it and achieves this in a manner which respects the humanity of the parents.”
 Announcing the expansion of the scheme, Children and Families Minister Edward Timpson MP said that since 2008, the FDAC had thrown an invaluable lifeline to hundreds upon hundreds of families and that extending its work would deliver life-changing results for families across the country.
Announcing the expansion of the scheme, Children and Families Minister Edward Timpson MP said that since 2008, the FDAC had thrown an invaluable lifeline to hundreds upon hundreds of families and that extending its work would deliver life-changing results for families across the country.
The court’s founder, District Judge Nicholas Crichton, said: “In the FDAC, we have seen some parents demonstrate a remarkable capacity to change in response to our more constructive, empathetic approach.
“Harnessing the fairness and authority of the court has shown that it is possible to break the cycle of drug and alcohol misuse.
“Importantly, FDAC has the support of parents themselves, which is crucial to its success.”
This extension should mean about a quarter of English family courts have an FDAC. However, there is concern that while hundreds of families may now go through FDAC every year, this will still represent only a very small proportion of the total number who could benefit.According to the court service Cafcass, more than 18,000 children were involved in care proceedings in England in 2013-14.
Cathy Ashley, Chief Executive of Family Rights Group, a charity which supports families whose children are the subject of local authority involvement, said she was a “big fan” of FDAC but that her concern was that “the numbers who will benefit from this roll out will be minuscule compared to the thousands of families going through care proceedings.”
She said she was also concerned that Government funding is only for one year, and progress might not be sustained.
Public Health England supports alcohol/drug services
Public Health England (PHE) has announced the successful applicants for £10 million of capital funding for services that are helping people in England with drug or alcohol problems to recover from their addiction. Over 50 projects across England, in partnership with local authorities, will receive grants from PHE.
PHE says that people recovering from addiction can have extremely limited skills or employment experience, and often have significant problems with unstable accommodation. Increasing evidence shows jobs and houses play a major role in successfully completing treatment from addiction. Out of the designated £10m capital funding, PHE has awarded a substantial proportion to projects that provide tailored education, training, skills and employment support to people in recovery, and to projects that provide safe and secure accommodation from which it’s possible to recover.
This is the second year that Public Health England has led a programme of £10m capital investment in drug and alcohol recovery services, following a successful programme in 2013-14, in which a range of innovative recovery-focused projects received funding.
Rosanna O’Connor, Director of Alcohol, Drugs and Tobacco at Public Health England said:
“I’m delighted that for a second year we can support an outstanding range of exciting and innovative local projects.
“Drug and alcohol misuse is a complex issue that causes significant harm to society. I am hugely encouraged by the level of commitment to improving recovery services, both from within the sector and among local authorities. These services will make a real difference to people in recovery, and communities across the country. I am particularly pleased that Public Health England is able to invest in services that will help people in recovery into work and to have a safe, supportive place to live.”
The full list of successful applications is available to view via the National Treatment Agency website, part of Public Health England.
Anti-binge drinking campaigns should promote benefits of abstinence
Pointing out the advantages and achievability of staying sober is more effective than traditional approaches that warn of the risks of heavy drinking, according to the research carried out at the University of Sussex, by researcher Dr Dominic Conroy.

The study, published in the British Journal of Health Psychology, found that university students were more likely to reduce their overall drinking levels if they focused on the benefits of abstaining, such as more money and better health.
They were also less likely to binge drink if they had imagined strategies for how non-drinking might be achieved – for example, being direct but polite when declining a drink, or choosing to spend time with supportive friends.
Typical promotions around healthy drinking focus on the risks of high alcohol consumption and encourage people to monitor their drinking behaviour (e.g. by keeping a drinks diary). However, the current study found that completing a drinks diary was less effective in encouraging safer drinking behaviour than completing an exercise relating to non-drinking.
Dr Conroy says: “We focused on students because, in the UK, they remain a group who drink heavily relative to their non-student peers of the same age. Similarly, attitudes about the acceptability of heavy drinking are relatively lenient among students.
“Recent campaigns, such as the NHS Change4Life initiative, give good online guidance as to how many units you should be drinking and how many units are in specific drinks.
“Our research contributes to existing health promotion advice, which seeks to encourage young people to consider taking ‘dry days’ yet does not always indicate the range of benefits nor suggest how non-drinking can be more successfully ‘managed’ in social situations.”
Dr Conroy studied 211 English university students aged 18-25 over the course of a month. Participants in the study completed one of four exercises involving either: imagining positive outcomes of non-drinking during a social occasion; imagining strategies required successfully to avoid drinking during a social occasion; imagining both positive outcomes and required strategies; or completing a drinks diary task.
At the start of the study, participants in the outcome group were asked to list positive outcomes of not drinking and those in the process group listed what strategies they might use to reduce their drinking. Those in the combined group did both.
They were reminded of their answers via email during the one-month course of the study and asked to continue practising this mental simulation.
All groups completed an online survey at various points, indicating how much they had drunk the previous week.
Over the course of one month, Dr Conroy found that students who imagined positive outcomes of non-drinking reduced their weekly alcohol consumption from 20 units to 14 units on average.
Similarly, students who imagined required strategies for non-drinking reduced the frequency of binge drinking episodes – classified as six or more units in one session for women, and eight or more units for men – from 1.05 episodes a week to 0.73 episodes a week on average.
Interestingly, the research indicates that perceptions of non-drinkers were also more favourable after taking part in the study. Dr Conroy says this could not be directly linked to the intervention but was an interesting additional feature of the study. He says: “Studies have suggested that holding negative views of non-drinkers may be closely linked to personal drinking behaviour and we were interested to see in the current study that these views may have improved as a result of taking part in a non-drinking exercise.
“I think this shows that health campaigns need to be targeted and easy to fit into daily life but also help support people to accomplish changes in behaviour that might sometimes involve ‘going against the grain’, such as periodically not drinking even when in the company of other people who are drinking.”
Dr Conroy collaborated on the paper with University of Sussex colleagues Dr Paul Sparks and Dr Richard de Visser.
Podcast
Our monthly podcast features interviews with experts from across the sector.
Gambling industry harms and parallels with the alcohol world
Will Prochaska –
Coalition to End Gambling Ads