
In this month’s alert
Cameron backs minimum pricing – But his Health Secretary disagrees
Prime Minister David Cameron has come out in support of minimum unit pricing of alcohol. It was reported in the Daily Telegraph over the Christmas period that the Prime Minister will overrule Cabinet colleagues to push through plans setting a minimum price. Officials have been ordered to draw up proposals for a 40-50p unit floor price in English shops and supermarkets. A Whitehall source told the newspaper: “The Prime Minister has decided that when it comes to alcohol, something pretty radical now has to be done and he is keen on the minimum price.” The source added: “It is complicated how this can be delivered, particularly under European law, but it is clear that the voluntary approach has not worked.”
Officials drawing up the new Alcohol Harm Reduction Strategy, expected to be published later in the year, have been told to re-visit the issue of alcohol pricing in view of the Prime Minister’s apparent wish to go a long way beyond the Coalition Government’s existing commitment to ban ‘below cost’ sales of alcohol, a policy which has been roundly condemned by the public health lobby, and even some industry groups, as inadequate to the task of tackling the problem of cheap alcohol.
However, it is clear that minimum pricing remains a controversial policy within government, as well as among Conservative MPs. Health Secretary, Andrew Lansley, has previously criticised minimum pricing as ineffective, and he has warned that such a move would not meet European competition rules. That view has been echoed by the Business Department and it is understood that the Treasury has received strong legal advice to that effect. Scotland’s administration is pushing through legislation for a minimum unit price, though Scottish Health Secretary Nicola Sturgeon admits it is “almost certain” to meet a legal challenge.
Problem of Cheap Alcohol
Prior to his comments to the Daily Telegraph, David Cameron had already accepted that cheap alcohol is a problem and he pledged to look “very carefully” at the issue of price controls for alcohol, ahead of the new Alcohol Strategy. The Prime Minister was speaking at Prime Minister’s Question Time on 14 December 2011, prior to a Parliamentary debate on alcohol taxation in Westminster Hall later that day. The debate was secured by Dr Sarah Wollaston MP, and was attended by the Economic Secretary to the Treasury, Chloe Smith MP. On the day of the debate, a group of leading health experts published a letter in the Daily Telegraph calling for the Government to take action and introduce stronger pricing policies to put an end to cheap drink sold at “pocket-money prices”. The letter was signed by 22 organisations and individuals, including the British Medical Association, the Royal College of Nursing and the IAS. At Prime Minister’s Questions in the House of Commons, Mr Cameron referred to the letter, saying: “I have no doubt in my mind that very low cost alcohol is part of the problem in our town centres… I note very carefully the letter that’s in the papers this morning from a whole set of people with great expertise about this and we’re looking very carefully at that issue.”
However, a few days later, Health Secretary, Andrew Lansley, gave an interview to the Sunday Independent in which he attacked the idea of minimum pricing of alcohol and argued that raising the price of alcohol ‘would do little to curb excess.’
The Debate
In her opening speech, Dr Wollaston outlined the importance of raising the price of cheap drink in order to reduce rates of health and social harm caused by alcohol. She said:
“Numerous studies around the world have shown public health benefits as a result of price increases and taxation policies, so is it not time for some evidence-based politics?”
Dr Wollaston argued that the Coalition Government’s current plans to introduce a floor price for alcohol that includes duty plus VAT will not deliver any “meaningful results”. Dr Wollaston added that the Coalition Government’s planned ban on ‘below cost’ sales of alcohol would only catch one in 4,000 of the drinks currently being sold “and would do nothing to save lives.” Dr Wollaston illustrated how easy it was to access cheap drink from a leading UK supermarket chain:
“Last weekend my researcher was able to access two litres of own-brand cider from Asda for £1.48, which worked out at just 18p per unit. With a four-pack of bitter for 68p, the price was just 17p a unit. I particularly objected to the labeling. It said, ‘Asda Smart Price’… there is nothing smart about charging 68p for four units of alcohol. That would send a woman well over the safe limit for a single day for just 68p.”
Dr Wollaston called upon the Government to investigate effective mechanisms for raising the price of cheap alcohol, including the introduction of a minimum price per unit, and a windfall tax for supermarkets.
Responding to the debate, Chloe Smith MP said that minimum unit pricing would be “incompatible with article 34 ….. of the European Union… That is the position.” The Economic Secretary to the Treasury also argued that the introduction of an indirect tax for supermarkets would be problematic to set up as “it would be difficult to distinguish between points of sale.” Miss Smith closed the debate by saying that “the Government are keen to hear evidence on the matter [of price]” and, in reference to the Scottish National Party’s intention to introduce a minimum unit price of alcohol, “will observe carefully what is going on in Scotland and elsewhere.”
Health Secretary opposes minimum pricing
In his interview in the Sunday Independent, Andrew Lansley said that there were “big problems” with the idea of minimum pricing, which he said would penalise the poor, fall foul of EU competition laws, and do little to tackle the kind of dangerous drinking seen in town and city centres on Friday and Saturday nights. He added that a minimum price of 50p per unit would hand £600m in extra revenue to drinks firms. Mr Lansley said: “Are we really saying that because a bottle of vodka isn’t £8 but £12.50 they are not going to preload with a bottle of vodka for a night out when they are in clubs where they pay £5 for a drink? That is absurd. They are still going to do this binge drinking because that is a behaviour issue. We have got to do much more to focus on what this means.”
He did concede that higher prices for drink can reduce consumption but added:
”It is more likely to have a bigger proportionate impact on responsible drinkers who happen to be low-income households.”
The Alcohol Strategy for England is due to be published in early 2012.
Health experts’ letter to the Telegraph
SIR – Today, MPs debate the crucial issue of alcohol taxation. Each year, alcohol causes the admission of over a million people to hospital, is linked to 13,000 new cases of cancer and is associated with one in four deaths among young people aged 15 to 24.
There is a wealth of evidence to show a direct correlation between alcohol affordability and levels of harm. The House of Commons Health Select Committee state: “increasing the price of alcohol is… the most powerful tool at the disposal of a government.” In 2010, alcohol was 44 per cent more affordable than it was in 1980, a trend mirrored by an increase in cases of alcohol-related health problems and social damage.
We urgently need to raise the price of cheap drink. Harmful drinkers and young people are likely to be the most responsive to price increases. In particular, we need to narrow the price gap between alcohol in bars and restaurants with alcohol in supermarkets and off-licences, to make bulk discounts and pocket-money prices a thing of the past.
There is a push towards a minimum price for each unit of alcohol in the devolved nations of the United Kingdom, with the SNP leading the debate in Scotland. This is a simple and effective mechanism for the Scottish Government to control alcohol prices. If the Coalition is not ready for such bold action, MPs must not lose sight of the importance of taxation as a means not only to lower alcohol consumption but also to direct revenue into the public purse.
With alcohol harm costing us an estimated £25 billion each year, MPs must act now.
Professor Sir Ian Gilmore, Chairman, UK Alcohol Health Alliance and Special Advisor on Alcohol, Royal College of Physicians
Dr Hamish Meldrum, Chairman, British Medical Association Council
Katherine Brown, Head of Research and Communications, Institute of Alcohol Studies
Andrew Langford, Chief Executive, British Liver Trust
Professor Lindsey Davies, President, Faculty of Public Health Professor
Jon Rhodes, President, British Society of Gastroenterology
Dr Dominique Florin, Medical Director, Medical Council on Alcohol
Professor Eileen Kaner, Institute Director and Professor of Public Health Research, Institute of Health and Society
Nick Barton, Chief Executive, Action on Addiction
Professor Humphrey Hodgson, Director, Institute of Hepatology, UCL
Professor Mark Bellis, Director, Centre for Public Health
Dr Peter Carter, Chief Executive and General Secretary, Royal College of Nursing
Dr Chris Record, Consultant Hepatologist, Newcastle University and Newcastle Hospitals NHS Trust
Dr Noel Olsen FRCP, FFPHM
Dr Jennifer R Lisle, Trustee, on behalf of the Royal Society for Public Health
Dr Marsha Morgan, Physician, University College London Medical School
Dr Evelyn Gillan, Chief Executive, Alcohol Focus Scotland
Dr David Snashall, Professor of Occupational Medicine, King’s College London and Honorary Consultant and Clinical Director, Occupational Health & Safety Services, Guy’s & St Thomas’ NHS Foundation Trust
Professor Peter Hayes, Ex President, British Society for the Study of the Liver and Professor of Hepatology, Scottish Liver Transplant Unit, Royal Infirmary of Edinburgh
Paul Lincoln, Chief Executive, National Heart Forum
Dr Bruce Ritson, Chairman, Scottish Health Action on Alcohol Problems
Eric Appleby, Interim Chief Executive of Alcohol Concern
Public sceptical of minimum pricing but only because they don’t understand it
The public are generally sceptical of the introduction of a minimum pricing policy, according to new research carried out for Alcohol Research UK. However, the researchers conclude that scepticism arises because many people do not fully understand the policy and its implications.
Many of those interviewed in the research project did not see the policy as targeting discounted alcohol sales, failed to recognise the public health significance of small population-level reductions in alcohol consumption, and were preoccupied with the effects for heavy and dependent drinkers.
When asked how the introduction of a minimum pricing policy might be made more acceptable, participants suggested that the money raised should be used to fund other interventions and that the policy should be introduced as part of a wider package of government policies to address excessive alcohol consumption.
The misconceptions highlighted by the research must be addressed, said lead researcher, psychologist Professor Martin S Hagger of Curtin University, Australia, if a minimum pricing policy is to be successfully introduced. Professor Hagger continued:
“As well as being sceptical about the effectiveness of a minimum pricing policy, many of those who took part in our research simply didn’t fully understand the policy and its implications. There are many ways in which the issue of alcohol-related harm could be tackled, but if the government chooses to implement a minimum pricing policy, our research suggests that it would be more acceptable to people if it were introduced as part of a wider package of measures to target excessive drinking. Policymakers must focus on communicating the policy clearly so that people understand its purpose”.
Alcohol Research UK
The research on minimum pricing was released to mark the launch of the new charity, Alcohol Research UK (ARUK), a new independent charity set up to tackle some of the problems created by alcohol misuse and provide robust, scientific evidence to guide policy and practice in the UK. ARUK is the successor to the body known as the Alcohol Education and Research Council.
Speaking about the launch, Professor Robin Davidson, Chairman of Alcohol Research UK, says: “This launch marks the beginning of a new era for research into alcohol-related harm in the UK. There is no doubt that excessive drinking can have a profoundly negative impact on both individuals and society. Alcohol Research UK is committed to funding research to help policymakers and practitioners make evidence-based decisions to help address this high-profile issue. This commitment is clear as we launch our new flagship grant programme, offering a grant of £300,000 to fund research which will help shape future policy and practice. We need to take action now to ensure the future of our society is not tarnished by alcohol misuse, and work with partners including Comic Relief and Drinkaware to achieve this objective. The launch of Alcohol Research UK is just the beginning – there’s a long way to go, but we aim to be on the front line, providing the research and information policymakers need to help them shape a positive future.”
Minimum pricing back on Scots agenda
A Bill to introduce minimum pricing of alcohol, as a condition of licences granted under the Licensing (Scotland) Act 2005, has been included in the Scottish Government’s programme for 2011- 2012. The actual minimum price will be specified in subordinate legislation. These measures will, hopefully, help to reduce alcohol consumption in Scotland and reduce the impact of alcohol misuse and over consumption on public health, crime, public services, productivity and the economy as a whole.
This would constitute something of an innovation in the UK. The chances of the Bill being passed are, of course, much greater, now that the SNP leads a majority Government. However, uncertainties remain, in regard to European law, and some of the big alcohol companies plan to oppose minimum pricing by referring the matter to the European Court as a breach of competition law.
Whether or not the move towards minimum pricing succeeds, the Scots Government programme will remain notable as the first occasion when a Government within the UK has committed itself to a policy of reducing national alcohol consumption.
Minimum pricing needed now more than ever
New report shows alcohol can be bought today for just 14p per unit 
Alcohol Focus Scotland and Scottish Health Action on Alcohol Problems (SHAAP) have published a report arguing that minimum unit pricing is needed now more than ever as alcohol continues to be sold at ‘pocket money’ prices.
The report, published jointly by alcohol agencies in Scotland and England, shows that, despite recent duty increases, alcohol is being sold for as little as 14p a unit in Scotland.
The report demonstrates how the alcohol industry uses price, place, promotion and product design to persuade customers that too much alcohol is not enough. Super-low prices are just one of the industry’s ‘tricks of the trade’ to get people to buy ever more alcohol. In supermarkets in Scotland within two weeks of publication of the report:
- Two cans of lager were sold for less than the price of a can of leading brand cola
- A young person receiving the average pocket money of £5.89 could buy 8 litres of cider containing 33 units of alcohol – enough alcohol to kill them
- Branded vodka was sold for 32p a unit – less than a can of leading brand cola
Dr Evelyn Gillan, Chief Executive of Alcohol Focus Scotland, said:
“We need minimum pricing now more than ever. Over the last few weeks, supermarkets have sought to undermine the new licensing legislation banning bulk discount buys by reducing the price of individual cans or bottles and encouraging online customers to buy cases of wine distributed from England. These antics make it clear that the big supermarkets are motivated by profit not public interest. This only serves to reinforce the case for government intervention through measures like minimum pricing if we want to reduce record levels of alcohol harm in Scotland. The vociferous opposition to minimum pricing by some of the big alcohol producers is reminiscent of the tactics the tobacco industry used to try to resist regulation which proved to be successful in saving lives. They should be seen for what they are – big business putting profits before health”.
Dr Bruce Ritson, Chair of SHAAP added:
“Abundant evidence shows the most effective way of reducing consumption and harm is increasing the price of alcohol relative to disposable income. Minimum pricing offers us the opportunity to save lives and protect communities from the devastating effects of harmful alcohol use. We know that minimum pricing is being discussed by Ministers in Wales and Northern Ireland and alcohol agencies in England are calling on Westminster to follow Scotland’s lead in introducing the policy. The coalition government’s favoured pricing measure of banning the sale of alcohol below the cost of duty and VAT will have virtually no effect on consumption and harm. Our colleagues in England are rightly looking to Scotland to lead the way in the UK and we hope the Scottish Parliament unites around this important piece of legislation.”
The report ‘Four Steps to alcohol misuse: how the industry uses price, place, promotion and product design to persuade us that too much alcohol is not enough’ is available for download at:
100 people a week die from alcohol-related liver disease in England and Wales
The rising toll of alcohol-related liver disease was highlighted by the British Liver Trust after mortality statistics for 2010 were released by the Office of National Statistics (ONS) showing an 11% increase in alcohol-related liver deaths since 2005. 4,609 people died from alcoholic liver disease, ICD code K70, in 2010, in comparison to 4,160 in 2005.
Andrew Langford, Chief Executive of the British Liver Trust, said: “With almost 100 people a week now dying from alcohol-related liver disease, it provides further compounding evidence to the debate that current strategies to tackle the problem are not working. We know that the lip service paid by the drinks industry and supermarkets through their empty promises, pledges and assurances are totally ineffective and I am genuinely concerned as to how many more deaths we have to face each year before any real, hard action is taken to tackle alcohol in the UK. Until we have robust strategies that address the real drivers of consumption like the pricing, advertising, availability and sponsorship of alcohol we won’t even begin to make a dent in these figures that are continuing to increase each year.”
The mortality statistics are obtainable from http://www.ons.gov.uk
Scots doctors warning about increased alcohol sales
Doctors’ leaders in Scotland called for tough action to tackle the cost of alcohol in Scotland following the release of information from Health Scotland that alcohol sales in Scotland had reached an all time high, surpassing volume sales in England and Wales. The Health Scotland report found that on average, this high volume of sales equated to 22.8 units of alcohol per adult, on average, per week, above the recommended upper weekly limit of 21 units for men.
Regular heavy alcohol consumption is known to have significant consequences for an individual’s health and a recent BMA survey of General Practices in Scotland found that, on one day in April, alcohol was a factor in more than 5,500 consultations in general practice in Scotland. This equates to around 1.4 million consultations per year, costing the NHS in excess of £28 million and accounts for 6% of all GP consultations.
The Scottish doctors’ leaders said that, while high volume sales of alcohol might be good for the drinks industry and supermarkets, alcohol harm costs Scottish taxpayers approximately £3.56 billion per year, around £900 per person. The cost of premature deaths caused by alcohol is estimated at £1.46 billion while healthcare-related costs are £268.8 million.
Dr Brian Keighley, Chairman of the BMA in Scotland, said: “In Scotland, the government has embraced the BMA’s policies on tackling alcohol misuse and has already legislated to improve licensing and end promotions to encourage bulk buying of alcohol in supermarkets. However, a failure by the Scottish Parliament to support minimum pricing means that it will be increasingly difficult to affect real change in people’s drinking habits. There is a wealth of evidence that demonstrates the link between price and consumption and this is a central part of any alcohol strategy…. It is essential that this parliament supports new legislation to introduce a minimum price for alcohol in Scotland. Sensible drinking begins with sensible pricing. The more alcohol that is sold in Scotland, the greater the numbers of people drinking to excess and the NHS will bear the brunt of the health consequences. The financial burden is no longer sustainable and if this trend continues the service will struggle to cope.”
“The most effective and evidence-based intervention to reduce consumption of alcohol is to tackle price and availability. Politicians have a central role in regulating the drinks industry and supermarkets to put an end to the ridiculous pricing of alcohol. By increasing price, we can reduce consumption and this, in turn, can prevent needless deaths.”
On one day in Scotland:
- alcohol will cost Scotland £97.5 million in terms of health, violence and crime
- alcohol will kill five people
- 98 people will be admitted to hospital with an alcohol-related condition
- 23 people will commit a drink driving offence 450 victims of violent crime will perceive their assailant to be under the influence of alcohol
The figures calculated by NHS Scotland from sales data show that, in 2009, the Scottish population aged 16+ consumed on average 1185 units of alcohol. The equivalent figure for England and Wales was 982 units. In all countries, around twice as many units of alcohol were purchased from off-licensed premises as from on-licensed premises –
Scotland, on-sales 386 units; off sales 799 units England and Wales, on sales 347 units, off sales 635 units
In both cases, the predominance of off-sales is probably not merely coincidentally related to the fact that the average cost of an off-sales unit of alcohol was less than half the price of an on-sales unit:
Scotland, on-sales, £1.28, off-sales 43p England and Wales on-sales £1.26, off-sales 44p
The combined cost of a unit of alcohol in Scotland was 71p, in England and Wales 73p. These figures do, of course, have implications for the argument about minimum pricing of alcohol. As, both north and south of the border, the average price of an off-sales unit of alcohol is already over 40p, it seems unlikely that minimum pricing would have significant impact on consumption levels unless the minimum unit price were set at at least 50p.
Ref: Alcohol Sales Data Scotland and England and Wales 1994- 2009. Healthscotland.com 2011
Scots re-thinking alcohol licensing
Call for separate alcohol checkouts and reduced trading hours
Scottish licensing boards should make more effective use of licensing legislation to control the overall availability of alcohol and reduce record levels of alcohol-related harm, according to a new report from Alcohol Focus Scotland.
The report also calls on the Scottish Government to take further action to regulate the sale of alcohol in off-sales and return licensing to its fundamental purpose of controlling the availability of alcohol to prevent harm.
Recommendations include:
Licensing policy should consider the overall effect of licensed premises on drinking behaviour and levels of harm in communities, not just the operation of individual licensed premises.
Off-sales hours should be reduced to 10am until 8pm.
Licensing boards should publish detailed information about the number, type and capacity of licensed premises in their area.
Separate alcohol-only checkouts should be introduced in supermarkets.
Licensed premises should be required to provide annual information on the volume of alcohol sold, by drink type, as a condition of their licence.
Licensing fees should be applied based on volume of alcohol sold.
Dr Evelyn Gillan, Chief Executive of Alcohol Focus Scotland, said: “Scotland is unique in having a licensing system that is based on protecting and improving public health. But we need to make sure that this principle is put into practice. The recommendations we are making today would shift the focus away from individual ‘problem’ licensed premises, to managing the overall availability of alcohol in the interests of society’s health and wellbeing. The licensing system exists because there is a consensus in society that alcohol is not an ordinary commodity. It is a substance with known toxic, intoxicating and addictive effects. As such, it needs to be carefully regulated.”
Dr Bruce Ritson, Chair of SHAAP, said:
“Licensing laws and practice have been steadily relaxed over the past 30 years with more licences issued to a wider range of premises and for longer opening hours. This greater availability has been associated with a substantial rise in alcohol consumption and harm. Over the past two decades, Scotland has had one of the fastest growing liver cirrhosis death rates in the world. Compared to other licensed or otherwise regulated products, alcohol stands out in being highly visible, accessible and aggressively promoted. If we want to reduce the record levels of alcohol harm we need to tackle the price and availability of alcohol.”
Epidemic of alcoholic liver disease in young people in North East England
The number of hospital admissions for people in their early 30s with alcoholic liver disease has increased by more than 400% in the North East of England in 8 years – the national increase stands at 61%.
Research carried out by Balance, the North East Alcohol Office, reveals that North East hospitals recorded 189 hospital admissions for 30-34 year olds with the disease last year, compared to just 37 in 2002.
In total there were 778 admissions for 30-34 year olds with alcoholic liver disease between 2002 and 2010, costing the NHS an estimated £1.8m. Disturbingly there were a further 482 admissions for under 30s, with some people admitted even being under the age of 20.
For all age groups, in the last 8 years there have been a total of 21,798 alcoholic liver disease admissions across the region at an estimated cost of £51.7m. Dr Chris Record, a liver specialist at Newcastle University and Newcastle Hospitals, said: “Only a few years ago alcoholic liver disease was very unusual in this age group and unless our drinking habits change, the problem is only set to worsen.
“The earlier the age at which children drink, and the more they drink, the greater the chance of developing serious liver disease in adult life. Many patients are now presenting with terminal liver disease in their late twenties and early thirties. Adults need to drink within the recommended limits and we need to discourage young people from drinking and perhaps even raise the legal age for alcohol consumption from below 5 to below 15. Unless we do something soon, liver specialists across the region are going to be dealing with more and more young people whose lives have been ruined by alcohol.”
Death rates linked to alcoholic liver disease have risen by over two-thirds (69%) in the last 30 years. The disease does not usually cause any symptoms until the liver has been extensively damaged, but starts with fat deposits in the liver leading to inflammation (steatohepatitis), fibrosis (scar tissue) and ultimately liver failure from cirrhosis. Alcohol also causes death from high blood pressure (hypertension), heart disease, stroke, pancreatic disease and cancer and, by directly damaging the brain, it frequently causes dementia at an early age. Dr Record added: “The body has remarkable powers of healing and it is never too late to stop drinking.”
Colin Shevills, Director at Balance, is calling for action to prevent this growing trend – starting with protecting children and young people from exposure to alcohol. Balance has launched a campaign which urges Government to prevent alcohol advertising on television, in the cinema unless it’s an 18 certificate film and to call a halt to the sponsoring of sporting and cultural events.
He said: “These figures are extremely worrying and demonstrate how starting to drink alcohol at a young age can have a serious impact on your health.
“Our region is drinking too much from an early age, driven by alcohol which is too affordable, too available and too heavily promoted. It is particularly concerning as, here in the North East, we have the highest rate of 11-15 years olds who drink in England and the highest rate of under18s admitted to hospital because of alcohol.”
To avoid health issues as a result of alcohol, adult drinkers are advised to stick to the recommended limits which are 2-3 units a day, or about two small glasses of wine, for a woman and 3-4 units, or about two pints of low strength beer or lager (3.5%), for a man and to avoid alcohol for 2 days after drinking more heavily than this.
Colin added: “We have created a society where alcohol plays too central a role in our lives. This needs to change. We are currently running a campaign to protect children and young people from exposure to alcohol through advertising, which encourages them to drink earlier and to consume more.
“Our campaign has already received support from thousands of North Easterners and they have signed our petition at www. balancenortheast.co.uk to restrict alcohol advertising and stop the detrimental effect it is having on young people and their health, both now and in the future.”
‘Stop recruiting North-east children as the next generation of drinkers’
‘Balance’ campaign against alcohol advertising
Alcohol advertising is risking the lives and futures of children across the North East by encouraging them to drink early and more, according to a campaign run in the north east of England. Through its ‘See What Sam Sees’ campaign, Balance, the North East Alcohol Office, is inviting North Easterners to take a child’s eye view and witness the way the alcohol industry is bombarding young people with ads which make drinkers appear popular, successful and attractive. In the region, 55% of people already agree that alcohol targets under 18s. Children and young people across the region are certainly being exposed. During the 2011 Rugby World Cup, which saw games broadcast during breakfast, children and young people in the North East were subjected to over 100 alcohol adverts. In one week, youngsters given permission to view the UEFA Champion’s League games saw alcohol ads in virtually every advertisement break.
The campaign is asking people to consider the damage that drinking too much, too young is doing across the North East. The campaign highlights that the region has:
The highest rate of alcohol specific hospital admissions for under 18s in England The highest rate of 11-15 year olds who admit to drinking alcohol
More than half of 15-year-olds who have drunk alcohol have experienced negative consequences including smoking, taking drugs and unprotected sex
Colin Shevills, Director of Balance, said: “Our children are brought up in a world where drinking at an early age and consuming large quantities is viewed as ‘normal’ or ‘acceptable’ and alcohol advertising plays a central role in this. We need to stop the alcohol industry from recruiting its next generation of drinkers and exposing young people to £800m worth of marketing a year.”
Balance TV ad banned
Central to Balance’s campaign is a film which follows Sam, a young boy, taking photographs of alcohol images during a normal day in his life. The photographs he has taken then flood the screen. However, the film cannot be viewed on TV after regulators said it contravened the Communications Act 2003 – due to the fact that Balance hoped to use the ad to encourage visitors to its website to sign a petition. The petition calls on Government to introduce more meaningful regulations to stop the alcohol industry reaching children and young people through advertising. Colin Shevells said: “We don’t object to the ruling in principle. However, it seems unfair that an advert which seeks to inform people and protect public health and the lives of our children is deemed unfit for broadcast. Meanwhile, the alcohol industry routinely flaunts the rules by making drinkers appear popular and attractive – something which it is not supposed to be able to do. “From our latest perception survey we also know that 68% of people in the North East agree that there should be a ban on alcohol advertising before 9pm. Balance is urging North Easterners to visit www.balancenortheast. co.uk and sign its petition which calls out for regulations to:
Prevent alcohol ads from targeting children and young people Prevent alcohol ads from being shown on TV and in the cinema for under 18 certificate films Prevent alcohol ads from being shown through social networking sites Prevent alcohol sponsorship of sporting and youth events
As part of the campaign, Balance has also been working with local schools to find out how alcohol advertising is affecting young people in the North East. The pupils aged from 14-17 were asked to emulate ‘Sam’ and take pictures of any alcohol advertisements they saw in their everyday lives. They were also asked how it made them feel. Pupils said they saw alcohol advertising ‘on the television, Youtube, Facebook, supermarkets, pubs’ and ‘magazines, bus stops, billboards, the internet’. They also said it made them feel that ‘alcohol is fun and you can’t have a good time if you don’t have a drink’. Colin added: “Sadly we live in a society where alcohol is too heavily promoted, too available and too affordable. It has become a dangerous part of our culture and it is obvious that the next generation is already being influenced by alcohol advertising at an early age. We need to protect our children and I hope people across the region will support our campaign.”
The Balance video is available to view at: http://www. balancenortheast. co.uk/our-campaigns/
School pupils “less tolerant” of drinking among peers, says new report, as smoking, drinking and drug use continue to decline
The latest figures on smoking, drinking and drug use among school children in England suggest that they are becoming less tolerant of drinking among their peers, while fewer are drinking, smoking or taking drugs. The figures, published by the NHS Information Centre, show that just under a third (32%) of 11 to 15-year-old pupils surveyed in 2010 said it was okay for someone their own age to drink alcohol once a week, compared to nearly half (46%) of pupils surveyed in 2003, the first year this question was asked. Meanwhile, around one in 10 (11%) thought it was okay to get drunk once a week, compared to one in five (20%) in 2003.
The findings are from Smoking, drinking and drug use among young people in England in 2010, which surveyed 7,300 pupils in September to December 2010 and shows a continuing decline in all three behaviours.
The 2010 survey focused on drinking and smoking and, for the first time, included responses to a new question about why pupils thought their peers drink. Pupils could select multiple answers and the most popular reasons given for peers’ drinking overall were:
- To look cool in front of friends (76%)
- Peer pressure from friends (62%)
- To be more sociable with friends (65%)
- For the buzz (60%)
However, there was a clear contrast in responses between pupils who drink and those who do not. The most popular reasons pupils thought their peers drank, among those who had drunk alcohol in the last week, were “for the rush or buzz” or “to be more sociable”. However non-drinkers thought their peers drank alcohol “to look cool in front of friends” or “because of pressure from their friends”.
The survey results also suggest an estimated six percentage point fall between 2009 and 2010 in the percentage of pupils who had tried alcohol; from 51 to 45%. This continues the downward trend since 2003, when 61% of pupils had drunk alcohol (similar to 2001 and 2002). However, the 2010 drop represents a greater fall than expected and future years’ data is needed to confirm if this is the start of a new trend.
The 2010 survey also shows:
- 27% of pupils had smoked at least once, compared to 44% in 2001
- 18% of pupils had reported having ever taken drugs, compared to 29% in 2001
Smoking, drinking alcohol and drug use are strongly associated with each other. Pupils who partake in one of these behaviours are more likely to partake in another.
Chief Executive of the NHS Information Centre, Tim Straughan, said “Our figures point to an increasingly intolerant attitude among young people in today’s society when it comes to the use of cigarettes, alcohol and drugs.
“As well as a reduction in the percentage who say they partake in these behaviours, a shrinking number think that drinking and drunkenness is acceptable among their peers.”
Poor parenting increases likelihood of binge drinking at ages 16 and 34
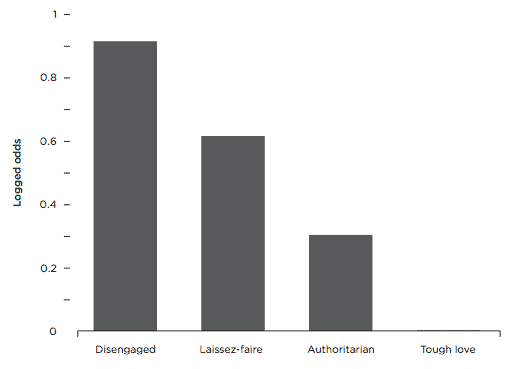
A study of over 15,000 children by the left-leaning think tank Demos shows parenting style is one of the most important and statistically reliable influences on whether a child ‘will drink responsibly in adolescence and adulthood’.
Demos found that ‘tough love’ parenting, combining consistent warmth and discipline, was the most effective parenting style to prevent unhealthy relationships with alcohol right into the mid-thirties age range.
The report, Under the Influence, funded by brewer SABMiller, is based on an analysis of data on over 15,000 children born in Great Britain over the last 40 years and followed up by the 1970 British Cohort Study (BCS), a large, well-respected longitudinal study of children and their parents in Great Britain.
The analysis found that:
- Bad parenting at age 10 makes the child twice as likely to drink excessively at age 34
- Bad parenting at age 16 makes the child over eight times more likely to drink excessively at that age
- Bad parenting at age 16 makes the child over twice as likely to drink excessively at age 34
The report also found that high levels of parental warmth and attachment at an early age and strict discipline at the age of 16 are the best parenting styles to reduce the likelihood that a child will binge-drink in adolescence and adulthood. While ‘tough love’ was the best parenting style to ensure against children becoming binge drinkers, less effective parenting styles were ‘authoritarian’, ‘laissez faire’ and ‘disengaged’.
Odds of excessive drinking at age 16 by parenting style when child was age 16
Binge-drinking figures in the UK have officially been dropping since the early 2000’s, but Demos argues that the culture of a binge drinking minority that has become more extreme, and more public, has fed the media’s infatuation with a ‘boozed-up Britain’.
Demos stresses that the lead role in how to deal with an entrenched binge culture needs to be taken by parents and government must support parents to do this. Without the active involvement of parents, policy to deal with binge drinking will not have the reach or impact desired to combat the problem.
Recommendations include:
For parents:
Discipline and supervision at age of initiation (15–16)
Strict discipline and supervision are extremely important at this age, for teaching children personal responsibility over the long term as well as protecting them from alcohol use and misuse in the short term. This holds true for both general parenting and alcohol-specific techniques. The evidence suggests that parents should not take a relaxed attitude to underage consumption, should discuss alcohol with their children within the context of setting firm boundaries, should avoid being drunk around their children and should actively ensure that their children develop sensible and responsible expectations of alcohol consumption.
Warmth during the early years (0–5) and up to the age of 10
Most parents will develop a warm and loving relationship in the early years of their children’s lives. The report stresses the importance of such a relationship for developing a number of extremely important life skills, including responsible drinking in later life.
Careful monitoring of alcohol access
Easy access to alcohol in the home is one of the key predictors of alcohol consumption and drunkenness among teenagers. Ensuring that alcohol in the home is monitored and that teenagers do not have access to it is an important element of a ‘tough love’ approach.
For Government:
Enforcement of under-age drinking laws
Discipline at 16 is an important mitigating factor against excessive alcohol consumption, even if it is not parent-led. By taking a strong line on enforcing the law of sales and proxy sales of alcohol to under-age drinkers, the government can help parents enforce alcohol boundaries by making it much harder for children to obtain alcohol. Such enforcement also helps strengthen the social norm that under-age drinking is not acceptable. Research shows that young people who buy their own alcohol are especially at risk of becoming problem drinkers.
Local partnerships to target trouble areas
Enforcement schemes can be effective if they are part of a broad local partnership of police, the local authority and retailers. Community alcohol partnerships, business improvement districts and Pub Watch are all examples of multi-component responses, where police, local retailers, local authorities and others work together to solve specific local alcohol-related problems such as under-age drinking or anti-social behaviour. The forthcoming alcohol strategy must contain a commitment to help these schemes.
Investment in alcohol-related school programmes that involve parents
Contrary to popular belief, evidence shows that teaching children specifically about alcohol and its dangers in school is not particularly effective at moderating their drinking behaviour. However, if the parents are involved, and the intervention deals with general life skills such as sociability, autonomy, application and so on, school-based programmes can be effective. The forthcoming alcohol strategy should ensure resources for school-based activities are targeted on these types of programmes. Where spending on alcohol reduction strategies does not clearly display effectiveness, it might be better to scrap symptom focused interventions and spend the money instead on evidence-based parenting programmes that are proven to work.
Spreading the six-week summer holiday throughout the year and providing activities for at-risk children
For children without engaged parents or in deprived communities the long summer holiday can provide opportunities to engage in risky behaviour like binge drinking. Structured activities can not only avoid boredom that leads to risky behaviour but can also provide inter-generational mixing that is crucial for young people’s positive development.
Jamie Bartlett, lead author of the report, said:
“The enduring impact of parenting on a child’s future relationship with alcohol cannot be ignored. This is good for parents: those difficult moments of enforcing tough rules really do make a difference, even if it doesn’t always feel like that at the time.
“While levels of binge drinking have fallen for five years running, there is a minority of extreme, publically visible, drinkers. No matter how high minimum pricing on alcohol is, there will be a hardcore of binge drinkers who will find a way to pay for it.
“For children whose parents may be disengaged, very practical measures, like spreading the school summer holiday throughout the year and providing activities for children in the school breaks, will go some way to preventing boredom and avoiding risky behaviour like under-age drinking.”
Under the Influence by Jamie Bartlett, Matt Grist and Bryanna Hahn can be downloaded free from www.demos.co.uk
Enforcement alone “won’t solve underage drinking problem”
Laws designed to tackle underage drinking are not being used to their maximum effect, according to a new report commissioned by the alcohol industry’s Portman Group.
The report, ‘Lost Orders?: Law Enforcement and Alcohol in England and Wales’ by Dr Fiona Measham, of Lancaster University, and research consultant Dr Phil Hadfield, enquires whether laws in the UK relating to the sale and consumption of alcohol are ‘fit for purpose’ and if they are being effectively enforced.

The study, based on interviews with 32 people working in key sectors, from pubs and clubs to magistrates’ courts and police forces, found evidence that some laws were considered impractical and were not being regularly enforced – for example, prosecutions against young people for underage drinking were particularly rare. But the research also concluded that enforcement alone would not solve the UK’s drinking problems.
Dr Fiona Measham said:
“In relation to certain offences, notably underage drinking, proxy sales and the serving of alcohol to intoxicated persons, our research found a clear propensity amongst enforcement agencies to target the suppliers of alcohol, rather than the consumers. In general, our interviewees regarded the prosecution of members of the public for breaches of the Licensing Act 2003 to be too expensive and time consuming to pursue. There was a perception that the courts would not support such prosecutions, or that the fines imposed would be minimal. Also, the commitment of resources required to obtain the necessary evidence for conviction was seen as disproportionately great.”
Dr Phil Hadfield said:
“One of the main messages of our findings is that there seems little point in Government introducing new tough sounding measures to tackle alcohol-related harms in the community if these laws are not actually enforced in practice. The rush to introduce new legislation has occurred at the expense of ensuring that the laws we already have are being implemented and effectively used.” The report concludes that enforcement is necessary, but not sufficient, in that it is unable to address the causes of unlawful or excessive demand for alcohol.
The research suggests that wide-ranging local partnerships – made up of agencies from police and primary care trusts to public transport providers and private security industry representatives – could be best placed to minimise harm from alcohol misuse.
Dr Measham said:
“We found enforcement powers alone could only operate as ‘sticking plasters’ to bigger challenges regarding the role of alcohol in British society, which individual agencies could not be expected to address. Shifting the legislative balance away from the current focus on crime and disorder and towards greater inclusion of health priorities was regarded as having clear benefits for partnership working. “For example, the more progressive agencies had adopted an ‘advise and educate’ approach in their dealings with licensed outlets, the aim being to establish relationships of trust wherein problems with customers could be reported without the fear of reprisals in terms of incidents being used as ammunition with which to review their license.
“Our research underlines the importance of allowing space for local innovation, with bespoke initiatives, in order to provide ‘local solutions to local problems’.”
Commercial pub crawls promote bingeing
New guidance codifies law enforcers’ powers to control pub/bar crawls
New research conducted by the Centre for Public Health, based at Liverpool John Moores University, found that commercially organised pub crawls for students, not surprisingly, appear to promote heavy drinking and sometimes illegal consumption, and are, naturally, accompanied by the health and social issues normally associated with bingeing.
Professor Mark Bellis, Director of the Centre for Public Health, and one of the authors of the report, commented:
“In September, tens of thousands of students will be initiated into university binge drinking cultures through pub-crawls or other alcohol promoting events. Most will be unaware that alcohol bingeing is one of the biggest killers of individuals of their age. The UK consistently leads Europe’s binge drinking tables but there is unlikely to be any change if the first part of a University education is a tutorial in extreme inebriation.”
The study
The researchers measured the drinking habits of students participating in commercially organised pub/bar crawls across England. They found that the scale of some larger events rendered organisers’ efforts to avoid negative consequences ineffective. A fifth (21%) of participants had illegally drunk alcohol in the street, despite street drinking bans, and the majority (87%) had consumed alcohol before joining the pub/bar crawl (pre-loading). Young adults consumed, on average, more than four times the government recommended daily unit guidelines for alcohol during the night – women typically drank around 13 units and men consumed 18 units. A follow-up survey found that 14% of participants reported hurting themselves, for example falling over, on the night.
The study, commissioned by the alcohol industry’s Drinkaware, was undertaken in response to increasing concerns about the health and social cost of events targeted at students. Informed by the results of the study, Drinkaware and the National Union of Students also commissioned the preparation of new guidance notes outlining the range of procedures and powers at the disposal of local authority licensing officers and police officers to manage safe pub/ bar crawls and reduce public nuisance.
Developed with the support of the Association of Chief Police Officers (ACPO) and the Home Office, the resource highlights the legal powers in the Licensing Act available to law enforcers to tackle issues relating to bar crawls and provides a model event organisers, law enforcers, universities and local partners can use to reduce the harm associated with pub/bar crawls. It recommends that organisers take greater responsibility for student safety and work more closely with venues and local law enforcement officers to prevent a good night turning bad.
Key recommendations include:
- Law enforcement officers, universities and student unions should share knowledge and experiences of commercial pub/bar crawls.
- In the planning stages, law enforcement officers should make bar crawl organisers and venues aware of their legal responsibilities and seek to identify and resolve anything which contravenes these.
- Local law enforcement officers should liaise with bar crawl organisers and venues to write a voluntary Bar Crawl Code of Conduct to ensure the safety and legality of an event, in the interests of both participants and the public.
- To limit the impact on local public services and avoid harm to participants, law enforcers should work with organisers to agree an upper limit on the size of bar crawls, appropriate to the area. Organisers should also be encouraged to arrange for all bar crawls to be supervised by first aid trained stewards.
Launching the new guidance, Pete Mercer, Vice President of Welfare at the NUS said: “As we see an increase in commercial bar crawls, it will be crucial for students’ unions, local police forces and councils to work together to minimise the detrimental impact they can have on the health and wellbeing of students, as well as on the local community.
“This practical guide for law enforcement officers is a welcome and responsible step forward in providing appropriate advice and support to ensure that students can enjoy their night out but also protect themselves and each other while they’re at it. It is equally vital that commercial organisers stop burying their heads in the sand and take their responsibility for the safety of students seriously.”
Alcohol guidelines should be reviewed
– No evidence to raise the limits – More emphasis on 2 days a week abstinence
MPs on the cross-party Science and Technology Committee have raised concerns about the advice offered by government in regard to the ‘sensible drinking’ limits. The Committee also concluded that greater efforts should be focused on helping people understand the guidelines and how to use them.
The Science and Technology Committee conducted an investigation into the alcohol guidelines in the light of any new evidence that had emerged since they were first formulated. Dr Marsha Morgan, representing the Institute of Alcohol Studies, was one of a number of expert witnesses to appear before the Committee. Others provided written evidence. There was a general consensus among the experts that no evidence had emerged to justify raising the drinking limits, but also that some confusion had arisen in the public mind about how the guidelines should be understood, particularly in regard to whether it was advisable to drink alcohol every day of the week, even within the limits. There was some disagreement among the experts in regard to the supposed health benefits of moderate drinking.
Andrew Miller MP, Chair of the Committee, said:
“Alcohol guidelines are a crucial tool for Government in its effort to combat excessive and problematic drinking. It is vital that they are up to date and that people know how to use them. Unfortunately, public understanding of how to use the guidelines and what an alcohol unit looks like is poor, although improving. While we urge the UK Health Departments to re-evaluate the guidelines more thoroughly, the evidence we received suggests that the guidelines should not be increased and that people should be advised to take at least two drink-free days a week.”
In 1987, the “sensible limits” for drinking were defined as 21 units of alcohol a week for men and 14 for women. By the early 1990s, scientific evidence had emerged suggesting that alcohol consumption might reduce the risk of coronary heart disease (CHD), prompting a review of the guidelines. The Government, therefore, recommended that drinking guidelines should be couched in daily terms: men should not regularly drink more than three to four units a day and women no more than two to three units a day.
Scepticism about health benefits
The Committee found a lack of expert consensus over the health benefits of alcohol and is, therefore, sceptical about using the purported health benefits of alcohol as a basis for daily guidelines for the adult population, particularly as it is clear that any protective effects would only apply to men over 40 years and post-menopausal women, yet the guidelines apply to all adults.
The Committee also found that, while public awareness of the existence of guidelines was high, a deeper understanding of what the guidelines were, and of what a unit of alcohol looked like, was lacking. Through the Public Health Responsibility Deal, the Government is working with the drinks industry to ensure that over 80% of alcoholic products on shelf will have labels with alcoholic unit content and the drinking guidelines by 2013.
The Committee concluded that the Government should remain mindful that sensible drinking messages may conflict with the business objectives of drinks companies, and should exercise proper scrutiny and oversight. The Government should conduct an interim assessment of the initiative in December 2012 rather than waiting for the target date of December 2013. The Committee also recommended that the Department of Health and devolved health departments should establish a working group to review the evidence and advise whether the guidelines should be revised.
The full report of the Science and Technology Committee can be downloaded from:
http://www.publications.parliament.uk/pa/cm201012/ cmselect/cmsctech/1536/153602.htm
“Nudging” on its own is unlikely to be successful in changing the population’s behaviour, says House of Lords Committee
The House of Lords Science and Technology Sub-Committee, in its report on Behaviour Change, concludes that there are important limits to what can be achieved by ‘nudging’, a non-coercive approach to encouraging healthier behaviour in the population favoured by the Coalition government.
The House of Lords report, the culmination of a yearlong investigation into the way the Government tries to influence people’s behaviour using behaviour change interventions, finds that ‘nudges’ used in isolation will often not be effective in changing the behaviour of the population. Instead, a whole range of measures – including some regulatory measures – will be needed to change behaviour in a way that will make a real difference to society’s biggest problems.
The House of Lords Committee thus joins the ranks of those criticizing the Coalition’s ‘Responsibility Deal’, the arrangements based around voluntary agreements with food, drink and other commercial operators to undertake actions intended to ‘nudge’ consumers into healthier behaviour.
The Coalition’s preference for a ‘nudge’ approach to improving public health, intended to contrast with an over-intrusive, ‘nanny state’ approach, has been roundly attacked by the political left and the health lobby for being ineffective and for giving corporate interests too much influence over health policy. However, the ‘nudge’ approach, like the Responsibility Deal itself, actually began life under the previous Labour Government. In its Labour incarnation, the Responsibility Deal was known as the ‘Coaltion for Better Health’ (See Alert, Issue 1 2011), and ‘nudging’ was advocated in a report ‘Mindspace’ commissioned by the Labour government.
House Of Lords Committee
Other findings and recommendations from the Committee include:
The Government must invest in gathering more evidence about what measures work to influence population behaviour change
They should appoint an independent Chief Social Scientist to provide them with robust and independent scientific advice
The Government should take steps to implement a traffic light system of nutritional labelling on all food packaging
Current voluntary agreements with businesses in relation to public health have major failings. They are not a proportionate response to the scale of the problem of obesity and do not reflect the evidence about what will work to reduce obesity. If effective agreements cannot be reached, or if they show minimal benefit, the Government should pursue regulation.
Committee Chair, Baroness Neuberger, said:
“There are all manner of things that the Government want us to do – lose weight, give up smoking, use the car less, give blood – but how can they get us to do them? It won’t be easy and this inquiry has shown that it certainly won’t be achieved through using ‘nudges’, or any other sort of intervention, in isolation.
“Behaviour change interventions are nothing new. Governments have tried to change our behaviour before – through legislation, marketing campaigns and even ‘nudges’, for example rumble strips on the road to get us to drive more slowly. And businesses also try to influence our behaviour all the time – supermarkets influence us though the location of, and promotions for, certain foods, and all businesses use advertising and marketing to change our behaviour.
“But focusing on how we can change a whole nation’s behaviour, has become an increasingly pressing issue as governments realise that societal problems, like the need to reduce obesity and reduce carbon emissions, aren’t going away – and are even getting worse. We welcome this Government’s desire to take the science behind behaviour change seriously in an attempt to find an effective solution.
“But changing the behaviour of a population is likely to take time, perhaps a generation or more, and politicians usually look for quick win solutions. The Government needs to be braver about mixing and matching policy measures, using both incentives and disincentives to bring about change. They must also get much better at evaluating the measures they put in place.
“In order to help people live healthier and happier lives, we need to understand much more about what sorts of policies will have an effect on how people behave. And the best way to do this is through research, proper evaluation of policies and the provision of well-informed and independent scientific advice.”
How many units in YOUR drink – BBPA unit-awareness poster campaign begins
The British Beer & Pub Association has revealed the first designs in a new national campaign to raise awareness among pubgoers over the number of units in their favourite drinks. The move follows a commitment under the new Public Health Responsibility Deal agreed between Government and alcohol retailers, with the BBPA pledging to promote much more visible alcohol unit information for consumers.
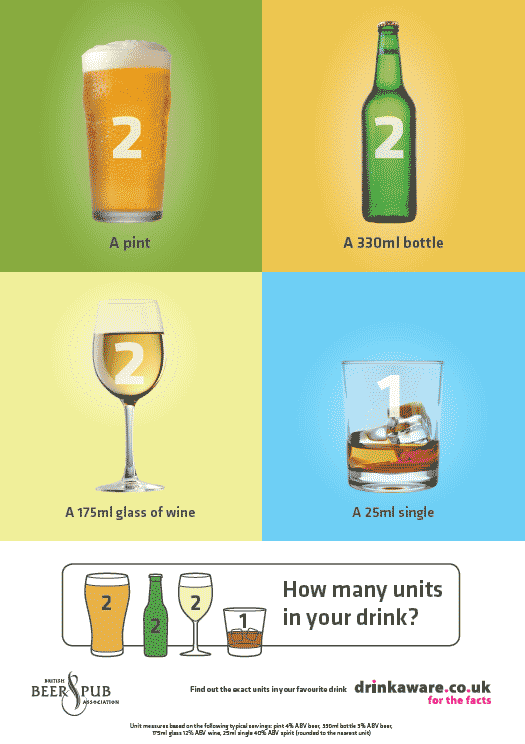
Newly designed posters, tent cards and beer mats featuring the slogan ‘how many units in your drink?’ are being piloted in selected BBPA member pubs over the summer, after which the materials will be available for pubs to order on a wider scale. The poster adopts a ‘2-2-2-1’ approach, to show the units in a typical pint of 4% abv beer, a typical 330ml bottle of 5% beer, a 175ml glass of 12% wine, and a 25ml single of a 40% spirit.
The final designs follow extensive research conducted with consumers and retailers in partnership with alcohol education charity Drinkaware. They reflect the research findings, which showed that pubgoers want clear information on the number of units in typical drinks in a way that presents the facts without adopting a nannying approach.
The BBPA says it has a strong track record in delivering successful awareness campaigns in pubs such as its Challenge 21 poster campaign which, in the past five years, has 90% recognition in its target group, according to polls.
Andrew Lansley MP, Secretary of State for Health, comments: “This is another example of the Responsibility Deal giving people the information to make their own choices about their health and lifestyle.
“Everyone should drink responsibly and within the recommended alcohol limits. Women should not regularly drink more than 2-3 units a day; and men should not regularly drink more than 3-4 units a day.
“I look forward to seeing the evaluation of this summer’s pilot and to a successful national roll-out to consumers across the country.”
Change4Life gives alcohol higher profile
The Coalition Government has unveiled its new Change4Life Three Year Social Marketing Strategy, up-dated to give alcohol a higher priority. Change4Llife is the brand name given to the health promotion campaign, originally focusing on the issues of diet, physical exercise and obesity. The alcohol component of the campaign has now been enhanced to support the government’s overall alcohol strategy when that is launched later in the year. Research conducted in 2010 to explore the potential for Change4Life to ‘stretch’ into topic areas beyond diet and physical activity found that the brand had the potential to operate closest to the increasing risk end of the spectrum and to encourage moderation as part of broader lifestyle changes.
Change4Life first introduced alcohol into its messaging via the adult launch commercial, ‘Alfie’ which encouraged adults, in a non-threatening way, to think about how their alcohol consumption might be affecting their health, and which was well received. However, it is known from qualitative research that many adults underestimate both the amount of alcohol that they drink and its potential to harm their health. People can be unwilling to confront the reality of how much they drink and may value the role alcohol plays in their life. In consequence, even when they are motivated to make changes to their lifestyles, alcohol tends to be the area chosen last. The Government has, therefore, decided to step up the alcohol-related component of Change4Life communication by:
- re-running the ‘Alfie’commercial
- introducing new communication that focuses on the health harms of alcohol
- encouraging parents to talk to their children about alcohol and alcohol health harms and to delay initiating their children into alcohol consumption until they are 15 (as recommended by the Chief Medical Officer for England)
Beyond what is covered by Change4Life, marketing will support the alcohol health harms strategy by:
- including messaging on binge drinking within the youth programme
- providing bespoke information for people living with conditions (as part of the activity targeting older people)
Tackling alcohol harm a priority for London
Tackling alcohol abuse, childhood obesity and cancer are the top priorities for a new partnership between the Mayor of London, London Councils and the NHS, to improve the health of all Londoners.
These key areas were agreed in a meeting of the London Health Improvement Board, launched early this year and backed by Andrew Lansley, Secretary of State for Health, signaling a new London-wide approach to health improvement.
The aim of the Board, chaired by the Mayor of London, and working in partnership with London Councils and the NHS, is to provide a London-wide approach on a number of key areas where an overall strategic focus is needed, in addition to the public health work already underway across the capital.
Mayor of London Boris Johnson said: ‘Through the London Health Improvement Board we have a fantastic opportunity for London to set the agenda about the issues that really matter to us as a city and to work together to ensure they are tackled. The paramount health problems that we must prioritise in London are obesity, particularly amongst children, alcoholism and its consequences, and awareness of cancers. During a time of economic strain, it is more important than ever that we join forces in this unique partnership to achieve tangible difference in these key areas.’
Cllr Colin Barrow, London Councils’ Executive Member for Health and Adult Services, said:
‘Londoners stand to benefit enormously from having a single body which will focus on driving through health improvements right across the capital. Real gains in health are made when different agencies work together and break down barriers to get the possible outcomes; this joint working not only makes the budgets go further, but can deliver significant gains, particularly in preventing more and make a real, chronic conditions. As local councils take on the new responsibilities for public health, we look forward to working with the Mayor and the NHS to add value to what is being delivered locally.’
Each year 27,000 Londoners are diagnosed with cancer and over a third of all Londoners will receive a cancer diagnosis at some point in their life. It is estimated that 280,000 Londoners are dependent on alcohol, levels among the highest in Western Europe and costing London £2.5 billion per year. Alcohol-related hospital admissions have increased by 124 per cent since 2003. The board today agreed that doing nothing is not an option when 72 per cent of Londoners are concerned about the impact of alcohol on their communities. The Mayor, London Councils and London’s NHS, are jointly committed to ensuring that support for individuals most at risk is in place and will be working with the relevant licensing authorities to make sure that alcohol is supplied responsibly.
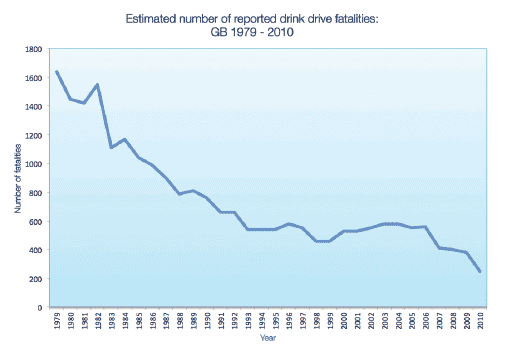
Remarkable fall in drink drive fatalities
Provisional drink drive estimates for 2010 show that fatalities resulting from drink and drive accidents fell by a remarkable 35% from 380 in 2009 to 250 in 2010, whilst seriously injured casualties fell by 18% from 1,490 to 1,230. Slight casualties resulting from drink drive accidents fell by 19% from 10,150 to 8,220. Total casualties also fell by 19% from 12,030 to 9,700. Fatal accidents decreased to 230 in 2010, a decrease of 3%. Overall drink and drive accidents fell by 18% from 8,050 to 6,630.
Some commentators have suggested that the apparent fall in drink drive deaths is so large that it may be too good to be true, and that when the final, confirmed figures are published they may be somewhat higher. However, even allowing for that possibility, it remains true that there has been a dramatic decline in the number of deaths from drink driving. Katherine Brown for the IAS commented:
“These figures are certainly an encouraging reflection of the declining trend in the number of drink drive incidents in the UK. However, the fact remains that hundreds of people are still being killed and thousands seriously injured on our roads each year by drivers who drink alcohol. Further steps need to be taken to reduce these unnecessary tragedies. Lowering the legal blood alcohol content and increasing police powers to breath test drivers are two policies that are proven to be effective in saving lives and have a great deal of support from the public, police, road safety and health communities. Disappointingly, the Government has chosen to ignore this evidence and will not be adopting these policies as part of its road safety strategy. However, the IAS will continue to advocate for their implementation as part of a cross departmental, evidence-based alcohol strategy.”
Announcing the results, Transport Minister Norman Baker said:
“These provisional figures show the number of people killed in drink drive accidents fell 35 per cent on the previous year – suggesting the number of drink drive deaths is now 83 per cent lower than 30 years ago. This is very welcome.
“However, we are determined to continue to take firm action against the small minority of drivers who still ignore the limit. That is why we are taking forward a package of measures to streamline enforcement against both drink and drug driving – including approving portable evidential breath testing equipment and drug testing devices which will speed up the testing process and free up police time.”
Counterfeit alcohol on the rise
An explosion which killed five men and severely injured a sixth on an industrial estate in Boston, Lincolnshire has brought to light a new kind of alcohol problem previously unknown in the UK. For it transpired that the explosion had taken place in an illegal distillery operated by Lithuanian migrant workers. Police investigating the incident discovered a filtration plant used for an illegal alcohol distilling process, along with three lorry-loads of counterfeit vodka, falsely labelled as Smirnoff.
Mass migration into the UK has resulted in approximately 25 per cent of the residents of Boston now coming from Eastern Europe, and it seems that it is largely foreign migrants who are behind the growth in the illegal alcohol trade, which is not restricted to Lincolnshire.
In the Spring of 2011, Her Majesty’s Revenue and Customs (HMRC) carried out raids to find out who was buying and selling the counterfeit vodka and to try to stop it reaching store shelves. As well as Boston, the raids also took place in Peterborough in Cambridgeshire, St Albans in Hertfordshire and Newcastle. HMRC is considering rolling out the operation nationwide after prosecutions in 16 cases, including one at a pub in Newcastle, successfully resulted in licences being revoked or suspended. In 2010, an illegal distillery run by Polish migrants was found in Hackney in north London. The distillery was producing two dozen bottles of counterfeit vodka every minute around the clock.
It is difficult to assess the precise dimensions of the illegal trade but estimates suggest that it could be costing the Treasury £millions a year in lost revenue. Channel 4 quoted a spokesman from the Department for Customs and Revenue as saying that in the period since 2005, HMRC have seized nearly 15 million litres of alcohol with a taxable value of over £33m and issued demands for more than £175m of evaded duty. However, the spokesman added that most illegal alcohol is smuggled, predominantly from Eastern Europe, rather than being the product of illegal distilleries in the UK.
What is clear is that counterfeit alcohol, smuggled or home made, can be even more toxic than the authentic products. Counterfeit products have been found to be adulterated with various chemicals including cleaning fluid, and methanol used in making anti-freeze. Speaking to Sky News, hospital Consultant Vikas Sodiwala said that a growing number of patients had been coming into accident and emergency at Lincoln County Hospital thinking their drinks had been spiked, when in fact they had drunk fake alcohol brands.
“It can be extremely dangerous,” he said. “The abdominal pain can be Mr Vikas Sodiwala severe, and they will need medication to get on top of that.” He said one possible outcome was permanent blindness. Mr Sodiwala added:
“It can also lead to liver failure, it can lead to kidney failure and it can ultimately lead to death.”
As the example of the Boston incident demonstrates, the illegal trade can also be highly dangerous for those involved in the production of the alcohol, not just the consumers.
NICE issues quality standard for alcohol misuse
The National Institute for Health and Clinical Excellence (NICE) has published a quality standard for the national health service on the treatment of alcohol dependence and harmful alcohol use.
The quality standard defines clinical best practice within this topic area. It provides specific, concise quality statements, measures and audience descriptors to provide the public, health and social care professionals, commissioners and service providers with definitions of high-quality care. The standard covers the care of children (aged 10-15 years), young people (aged 16-17 years) and adults (aged 18 years and over) drinking in a harmful way and those with alcohol dependence in all NHS-funded settings. It also includes opportunistic screening and brief interventions for hazardous and harmful drinkers. The quality standard addresses the prevention and management of Wernicke’s encephalopathy but does not cover the separate management of other physical and mental health disorders associated with alcohol use. The main elements of the standard are:
- Health and social care staff receive alcohol awareness training that promotes respectful, nonjudgmental care of people who misuse alcohol.
- Health and social care staff opportunistically carry out screening and brief interventions for hazardous and harmful drinking as an integral part of practice.
- People who may benefit from specialist assessment or treatment for alcohol misuse are offered referral to specialist alcohol services and are able to access specialist alcohol treatment.
- People accessing specialist alcohol services receive assessments and interventions delivered by appropriately trained and competent specialist staff.
- Adults accessing specialist alcohol services for alcohol misuse receive a comprehensive assessment that includes the use of validated measures.
- Children and young people accessing specialist services for alcohol use receive a comprehensive assessment that includes the use of validated measures.
- Families and carers of people who misuse alcohol have their own needs identified, including those associated with risk of harm, and are offered information and support.
- People needing medically assisted alcohol withdrawal are offered treatment within the setting most appropriate to their age, the severity of alcohol dependence, their social support and the presence of any physical or psychiatric comorbidities.
- People needing medically assisted alcohol withdrawal receive medication using drug regimens appropriate to the setting in which the withdrawal is managed in accordance with NICE guidance.
- People with suspected, or at high risk of developing, Wernicke´s encephalopathy are offered thiamine in accordance with NICE guidance.
- Adults who misuse alcohol are offered evidence-based psychological interventions, and those with alcohol dependence that is moderate or severe can, in addition, access relapse prevention medication in accordance with NICE guidance.
- Children and young people accessing specialist services for alcohol use are offered individual cognitive behavioural therapy, or if they have significant comorbidities or limited social support, a multicomponent programme of care including family or systems therapy.
- People receiving specialist treatment for alcohol misuse have regular treatment outcome reviews, which are used to plan subsequent care.
The full quality standard can be downloaded from http://www.nice.org.uk/ guidance/qualitystandards/ alcoholdependence/home.jsp
Podcast
Our monthly podcast features interviews with experts from across the sector.
Gambling industry harms and parallels with the alcohol world
Will Prochaska –
Coalition to End Gambling Ads